

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 3, June 2023, pages 211-220

A Prospective, Randomized Open-Label Study for Assessment of Antihypertensive Effect of Telmisartan Versus Cilnidipine Using Ambulatory Blood Pressure Monitoring (START ABPM Study)
Rahul Sawanta, Sachin Suryawanshib, Mayur Jadhavb, c, Hanmant Barkateb, Sumit Bhushanb, Tanmay Raneb
aHridaymitra Cardiac Clinic, Pune, Maharashtra, India
bDepartment of Global Medical Affairs, Glenmark Pharmaceuticals Ltd., Mumbai, Maharashtra, India
cCorresponding Author: Mayur Jadhav, Department of Global Medical Affairs, Glenmark Pharmaceuticals Ltd., Mumbai, Maharashtra, India
Manuscript submitted February 6, 2023, accepted April 25, 2023, published online May 26, 2023
Short title: START ABPM Study
doi: https://doi.org/10.14740/cr1476
| Abstract | ▴Top |
Background: The antihypertensive agent telmisartan is an angiotensin II receptor blocker with a terminal elimination half-life of 24 h and has a high lipophilicity, thereby enhancing its bioavailability. Another antihypertensive agent, cilnidipine is a calcium antagonist and has dual mode of action on the calcium channels. This study aimed at determining effect of these drugs on ambulatory blood pressure (BP) levels.
Methods: A randomized, open-label, single-center study was conducted during 2021 - 2022 on newly diagnosed adult patients with stage-I hypertension, in a mega city of India. Forty eligible patients were randomized to telmisartan (40 mg) and cilnidipine (10 mg) groups, with once daily dose administered for 56 consecutive days. Ambulatory blood pressure monitoring (ABPM) (24 h) was performed pre- and post-treatment, and the ABPM-derived parameters were compared statistically.
Results: Statistically significant mean reductions were observed in all BP endpoints in telmisartan group but only in 24-h systolic blood pressure (SBP), daytime and nighttime SBP, and manual SBP and diastolic blood pressure (DBP) in cilnidipine group. The mean change from baseline to day 56 between two treatment groups showed statistical significance in last 6-h SBP (P = 0.01) and DBP (P = 0.014), and morning SBP (P = 0.019) and DBP (P = 0.028). The percent nocturnal drop within and between groups was statistically nonsignificant. Also, the between group mean SBP and DBP smoothness index differed nonsignificantly.
Conclusions: Telmisartan and cilnidipine once daily were effective and well tolerated in the treatment of newly diagnosed stage-I hypertension. Telmisartan provided sustained 24-h BP control and may offer advantages over cilnidipine in terms of BP reductions, particularly over the 18- to 24-h post-dose period or critical early morning hours.
Keywords: Ambulatory blood pressure; Nocturnal dip; Smoothness index; Hypertension
| Introduction | ▴Top |
Hypertension is a common non-communicable disease (NCD) and is of major public health concern accounting for 19% of all deaths globally [1]. Hypertension is defined as an office blood pressure (BP) reading of at least 130 mm Hg systolic and 80 mm Hg diastolic, with the corresponding 24-h ambulatory BP readings being 125 mm Hg systolic and 75 mm Hg diastolic [2]. Today, an estimated 1.28 billion adults in the age range of 30 - 79 years worldwide have hypertension and two-thirds of them are living in lower- to middle-income countries. Nearly 46% of adults with hypertension are unaware of the condition, while about 42% of the cases are diagnosed and treated. Only about 21% of the cases have hypertension under control [3]. In India, hypertension is diagnosed if office BP exceeds 140/90 mm Hg and ambulatory BP exceeds 130/80 mm Hg, as per Indian guidelines on hypertension-IV [4]. The asymptomatic nature of hypertension contributes to a lack of awareness of this condition, thus being labeled as a “silent killer disease”. It is an independent risk factor for coronary heart disease, stroke, myocardial infarction, heart failure, and chronic kidney disease. If hypertension remains undiagnosed or uncontrolled, it can cause mortality or permanent disability [5]. However, it is a modifiable risk factor with non-pharmacological and pharmacological measures providing a substantial reduction of these conditions. Hence, BP measurements are essential for the diagnosis and management of hypertension [6].
The office (clinic) BP measurements provide a snapshot of an individual’s BP, which might be falsely elevated or falsely low [7]. Moreover, these measurements do not provide variations in BP during the day and the effect of antihypertensive treatment, which is essential for the management of hypertension. Ambulatory blood pressure monitoring (ABPM) allows the automatic reading of the circadian variation in BP and the evaluation of treatment efficacy throughout the dosing interval [8]. ABPM provides an effective prediction of cardiovascular risk and enables BP control at the time of heightened risk, thereby improving the long-term prognosis [9]. It helps in reducing the possible number of false readings and provides dynamic variations in BP [6].
To achieve effective control of BP, a long-acting antihypertensive agent is essential. Telmisartan is one of the angiotensin II receptor blockers (ARBs) with a terminal elimination half-life of 24 h and has a large volume of distribution due to its high lipophilicity [10]. This enhances its tissue penetration, intracellular absorption, and bioavailability. Telmisartan blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor in many tissues, such as vascular smooth muscle and the adrenal gland. Telmisartan does not bind to or block other hormone receptors or ion channels known to be important in cardiovascular regulation. The efficacy of telmisartan as monotherapy has been extensively studied using ABPM to demonstrate its BP control at the end of a once-daily dosing interval [11].
Another antihypertensive agent cilnidipine is a novel calcium antagonist due to its dual mode of action on the calcium channels. Cilnidipine blocks both the L-type and N-type calcium channels. Simultaneous blockade of the L-type and N-type calcium channels results in a significant reduction of BP without causing reflex tachycardia. It blocks the N-type channel at sympathetic nerve ending [12-14]. Thus, the dual mode of action of cilnidipine permits vasodilation and sympathetic blockade. Due to its lipophilic and avidly binding property, cilnidipine has shown prolonged and desirable antihypertensive effect [15].
Both telmisartan and cilnidipine are recommended as first-line drugs for hypertension control; however, the half-life of cilnidipine is shorter than telmisartan. Accordingly, a clinical trial was planned to evaluate if there is any difference in the 24-h antihypertensive efficacy of two drugs due to difference in half-lives, using ABPM. Moreover, the interest in the trial was to compare the safety and tolerability of telmisartan and cilnidipine administered to hypertensive patients.
| Materials and Methods | ▴Top |
Study design and participants
A prospective, randomized, open-label, single-center trial for assessing the 24-h antihypertensive efficacy of telmisartan versus cilnidipine was planned during the year 2021 - 2022. Newly diagnosed adult patients of either sex with stage-I hypertension and willing to participate in the trial were considered for screening. The demographics, vital signs, physical examination, and medical history were recorded for each participant. Moreover, blood samples were collected, and electrocardiogram (ECG) was recorded for each participant. Subjects with systolic blood pressure (SBP) ≥ 140 mm Hg and/or diastolic blood pressure (DBP) ≥ 90 mm Hg by manual cuff sphygmomanometer in clinical setup, requiring initiation of antihypertensive medication with single-drug therapy, were included in the study. Those subjects with hepatic impairment, chronic renal failure, and coronary artery disease were excluded from the study. Furthermore, type 2 diabetes mellitus (DM) patients diagnosed for more than 2 years, type 1 DM patients, patients with a history of surgery or malignant hypertension, recent substance abuse, breast-feeding or pregnant females, patients with history of human immunodeficiency virus (HIV) infection, hepatitis B and C were excluded from the study.
Randomization and masking
Forty eligible subjects were equally assigned to two groups/arms using a unique randomization code sequentially through an interactive web response system (IWRS). Subjects received one of the two active study drugs (i.e., either telmisartan 40 mg tablet or cilnidipine 10 mg tablet) based on randomization. The study medications were labeled with a unique material code that was linked with the randomization scheme. Randomization codes assigned to subjects were available to the investigator(s) from the IWRS without revealing the treatment allocation.
Procedure and investigational product (IP) administration
The study protocol has been schematically shown in Figure 1. Proper instructions regarding the device handling were given to each subject. On day 1, (24 h post ABPM device attachment), the subject visited the site to return the device and the data were extracted from the machine and stored in the computer as the pre-treatment data. Before the start of dosing, trough manual BP was measured manually. The study drug was dispensed to the subjects after detaching the ABPM device. They were instructed about the timings of IP intake for the entire duration of the study until the next visit. Subjects were administered with tablet telmisartan 40 mg (80 mg if needed) orally once daily, or cilnidipine 10 mg (20 mg if needed) orally once daily for 56 consecutive days (8 weeks). No other antihypertensive medications, apart from study drugs, were allowed during the study period. Subjects were asked to visit the site for applying the ABPM device on day 56 (end of study (EOS)) after the treatment period. The manual trough BP was measured immediately before the subject takes medication on day 56. On day 57, the device was detached from each subject and the data were downloaded to the personal computer. The BP recording times were similar at both day 0 and day 56, to compare the effect of treatment within and between groups. The vital signs and lab investigations (hemoglobin A1c (HbA1c), creatinine, urea, complete blood count (CBC) and bicarbonate) were also performed on day 57. The subject’s compliance, IP accountability, and assessment of adverse events (AEs) and serious adverse events (SAEs) were also done on day 57. Loss to follow-up was considered as subjects participating until the baseline visit but not attending subsequent visits. Informed consent was obtained from each patient and the Ethics Committee approvals were obtained before study initiation.
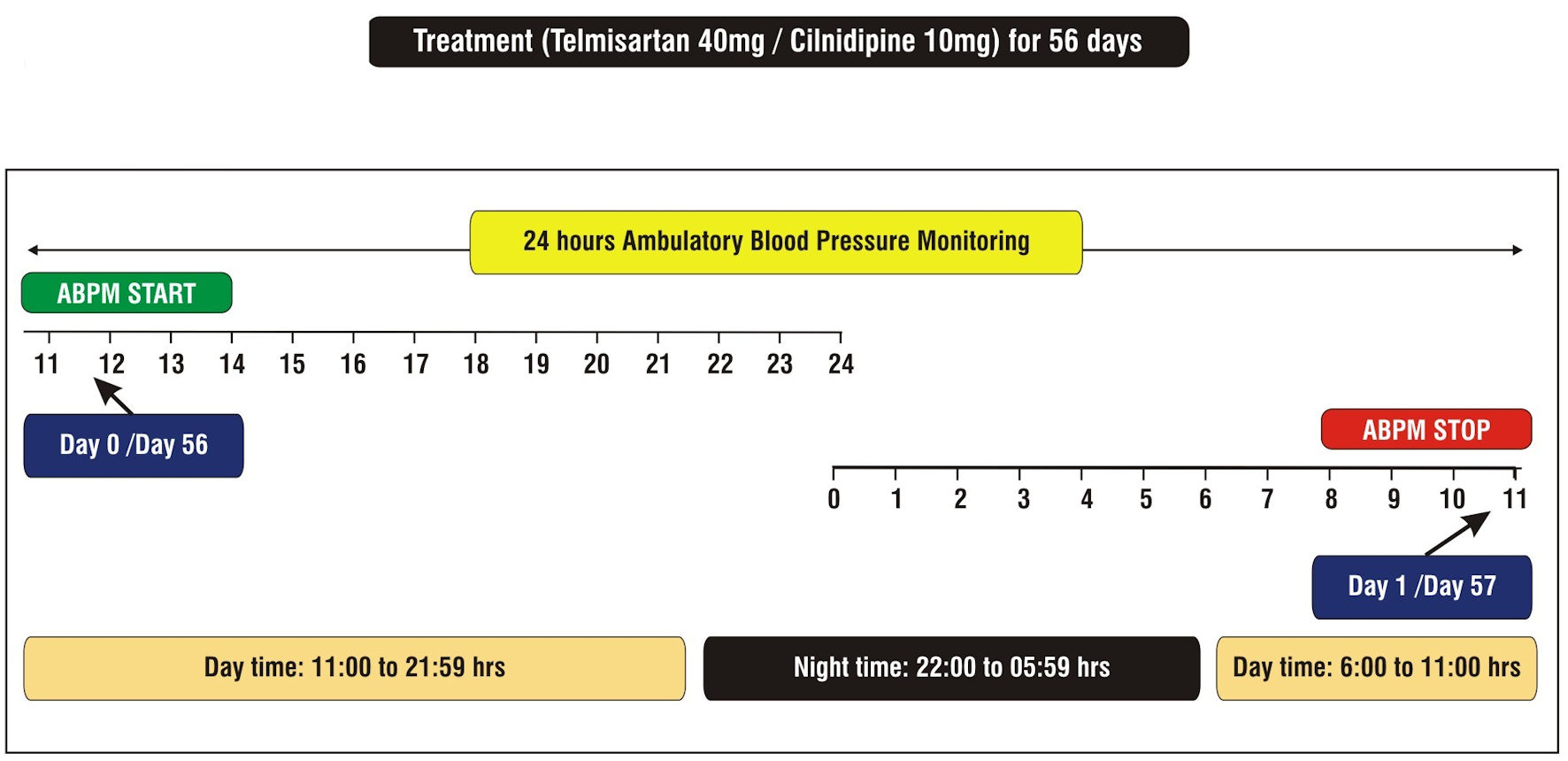 Click for large image | Figure 1. Schematic of study design. ABPM: ambulatory blood pressure monitoring. |
Efficacy and safety assessment
The efficacy of treatment was measured in terms of: 1) changes from baseline (day 0) to EOS (day 56) in mean SBP and DBP during the last 6 h of the 24-h dosing interval measured by ABPM; 2) changes from baseline to EOS in the mean SBP and DBP during the morning (06:00 to 11:59 h), daytime (06:00 to 21:59 h) and night time (22:00 to 05:59 h), as measured by ABPM; 3) changes from baseline to EOS in the mean seated trough SBP and DBP as measured by manual cuff sphygmomanometer; 4) BP responder rates; 5) nocturnal dip; and 6) smoothness index (SI) for SBP and DBP based on 24-h ABPM. The safety was assessed based on the incidence of AEs, SAEs and lab investigations. All the analyses were performed on the per-protocol population with at least 80% of the ABPM data on day 0 and day 56. All subjects receiving at least a single confirmed dose of the study drug and at least one post-baseline safety assessment were included in the safety analysis.
Data quality assurance
The study monitor reviewed the electronic case report forms (eCRFs) for accuracy and completeness during the on-site monitoring visits. Data queries were resolved with the investigator as needed. The data were transcribed into the eCRF. The investigator was responsible for the accuracy and adequacy of all data entered in the eCRFs.
The study was reviewed by the Institutional Ethics Committee (IEC) at the investigator site and was initiated after proper approval from EC. The trial was registered with protocol number IIS/2021/01. The entire execution of the study was as per the Declaration of Helsinki.
Statistical methods
The demographic parameter age and the anthropometric parameters were expressed in terms of mean, standard deviation (SD), and 95% confidence limits. The statistical significance of the difference in means was tested using a t-test for independent samples. The homogeneity of the sex distribution in the two groups was tested using Pearson’s Chi-square test. The 24-h ABPM data on patients were used to derive the following variables: 1) 24-h SBP and DBP; 2) systolic and diastolic last 6 h BP; 3) systolic and diastolic morning BP (06:00 - 11:59 h); 4) systolic and diastolic daytime BP (06:00 - 21:59 h); and 5) systolic and diastolic night time BP (22:00 - 05:59 h). The “bp” library from R-programming tools (version 3.4.3) was used to generate data on these variables. The in-built function in the library was used to read the instrument output resulting in a structured time-based data on BP parameter for each patient. The data were used in deriving new variables of interest by writing a customized script. Descriptive statistics like mean, SD, minimum and maximum were obtained for each variable at baseline and at day 56 using individual measurements. The comparison of mean values between the two groups at baseline was performed using a t-test for independent samples. The within-group comparison of each variable from baseline to day 56 was performed using paired t-test. The mean difference was tested for statistical significance against the hypothetical value of 0.
BP responders
The BP responders were defined based on the ABPM data as well as manual measurement data. For ABPM, a responder was defined as a subject with a mean 24-h DBP < 80 mm Hg or reduction in DBP at day 56 from baseline of ≥ 10%; and SBP < 130 mm Hg or reduction in SBP at day 56 from baseline of ≥ 10%. For manual measurement, the responder was defined as a subject with a mean DBP < 90 mm Hg or reduction in DBP at day 56 from baseline of ≥ 10%; and SBP < 140 mm Hg or reduction in SBP at day 56 from baseline of ≥ 10%. The distribution of responders and non-responders was compared between two groups using Pearson’s Chi-square test.
Nocturnal dip
The systolic and diastolic nocturnal dips were obtained as the percentage drop in the mean BP from daytime to sleep periods. The comparison of nocturnal dips between baseline and day 56 in each group was performed using paired t-test, while the change in dip from baseline to day 56 between the two groups was compared using a t-test for independent samples.
SI
The systolic and diastolic SI was derived from the ABPM data for each patient referring to baseline and day 56 hourly values. For each patient, the continuous BP data at baseline and day 56, on systolic/diastolic parameters, were partitioned into four time zones, viz. morning, afternoon, evening, and night times. The mean BP values were obtained at baseline and day 56 according to time zones for each patient. The difference of means between baseline and day 56 for each time zone was obtained. The ratio of the mean of these differences and the SD of differences was referred to as the SI for the patient. Both systolic and diastolic smoothness indices were obtained for each patient. Descriptive statistics like mean, SD, median and interquartile range for SI were obtained. The mean systolic/diastolic SI for both treatments was compared using a t-test for independent samples.
All the above analyses were performed using the R-programming tool (version 3.4.3) and SPSS, version 26.0 IBM Corp, USA, and the statistical significance was evaluated at 5% level.
| Results | ▴Top |
A total of 73 patients were screened, out of which 33 failed the inclusion criteria, thus leaving 40 patients for randomization. Twenty patients were randomized per group. During follow-up, one patient was lost in each group. Further, the continuous BP monitoring data for two patients in the telmisartan group were incomplete due to missing values, and hence were dropped from the analysis set. The final analysis was performed on 17 patients from the telmisartan and 19 patients from the cilnidipine group (Fig. 2). The per-protocol analysis was performed on the final data set. Table 1 provides descriptive statistics for demographic and anthropometric parameters of patients in two treatment groups. The mean age of patients in the telmisartan group was 41.88 (SD: 11.16) years, while that of the cilnidipine group was 41.47 (SD: 12.69) years, and the difference between the groups was statistically nonsignificant (P = 0.651). Further, the sex distribution, anthropometry, and clinical evaluations were also nonsignificantly different between the two at baseline (day 0). The ABPM data were obtained on these patients at baseline and day 56. Figure 3 provides the mean SBP and DBP profiles for 24-h duration at baseline and day 56 for both groups.
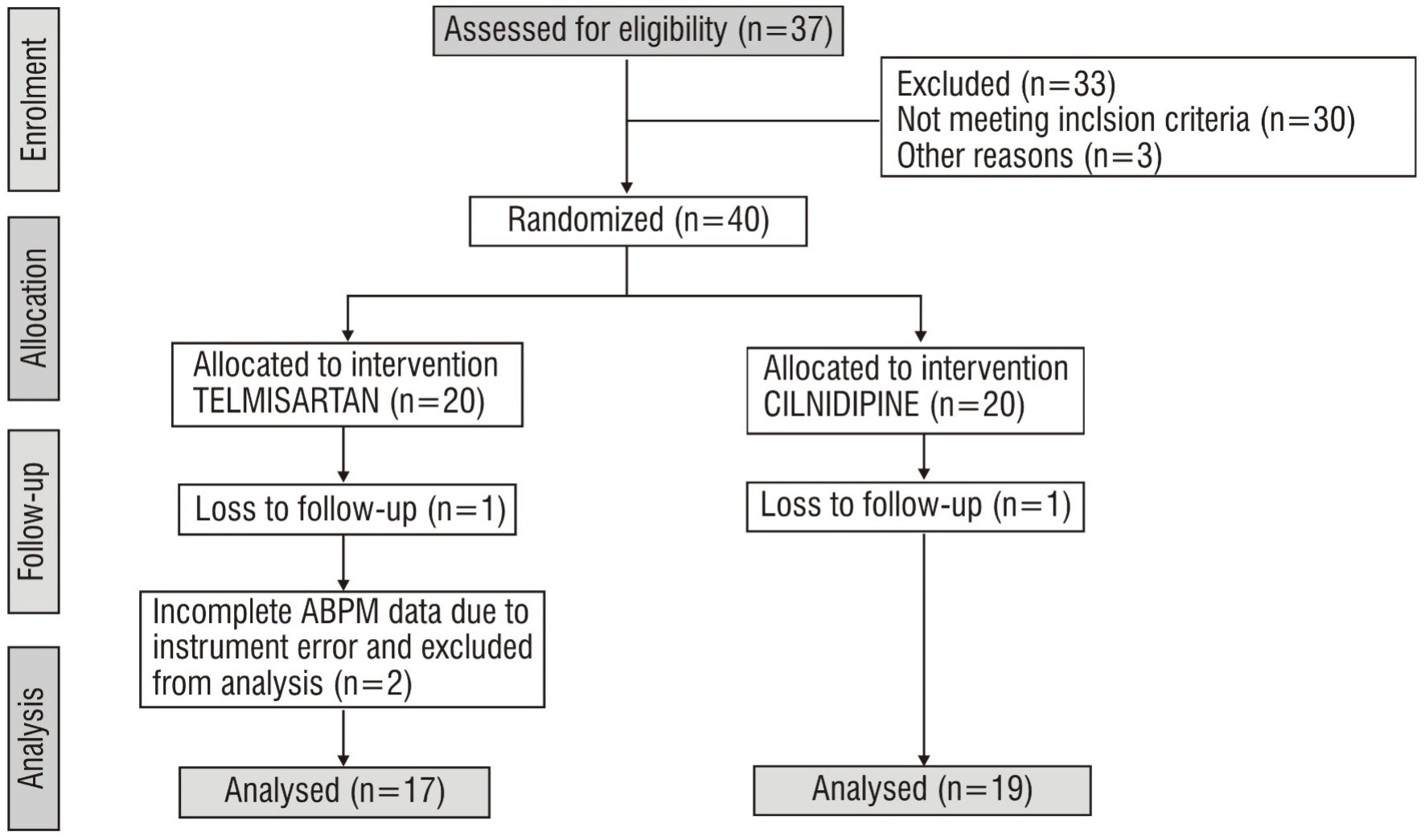 Click for large image | Figure 2. Sample flow diagram. ABPM: ambulatory blood pressure monitoring. |
 Click to view | Table 1. Baseline Characteristics of Subjects in Two Groups |
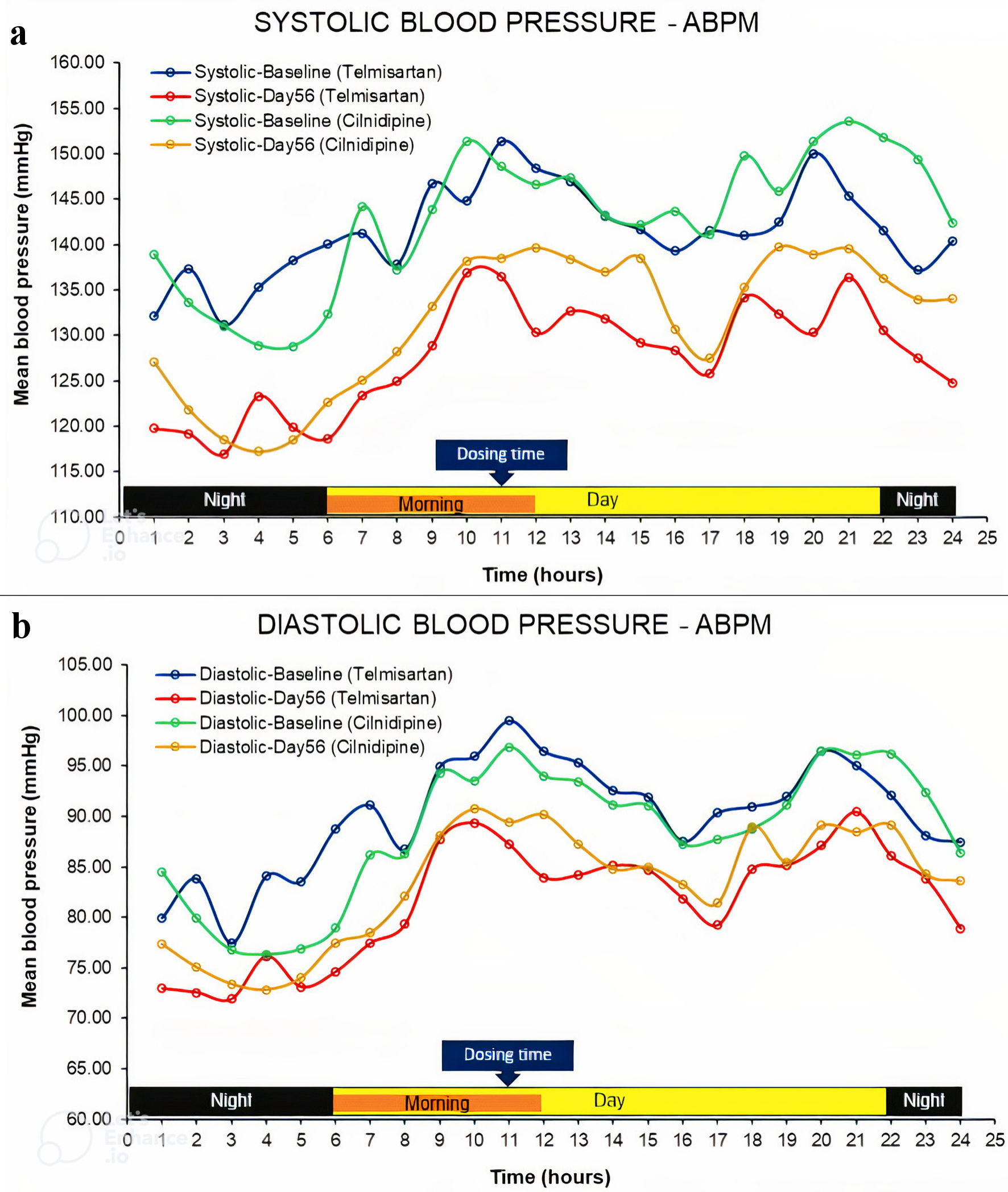 Click for large image | Figure 3. Profile of systolic and diastolic blood pressures during 24 h according to ABPM device. ABPM: ambulatory blood pressure monitoring. |
Table 2 provides descriptive statistics for various ABPM-derived variables and their comparison within the group. It also provides the change in variables from baseline to day 56 and the comparison of change between the two groups. In the telmisartan group, all the variables showed statistically significant mean differences, as indicated by P values < 0.05. In the cilnidipine group, systolic 24-h BP, systolic daytime BP, systolic nighttime BP, and manual systolic and diastolic measurements showed statistically significant mean differences with P values < 0.05. Further, the change in each variable from baseline to day 56 was compared between the two groups. The difference of means for systolic last 6 h (P = 0.010), diastolic last 6 h (P = 0.014), systolic morning (P = 0.019), and diastolic morning BP (P = 0.028), showed a statistically significant difference between the groups. The mean change in the telmisartan group was significantly higher than that in the cilnidipine group. The nocturnal dip was also analyzed for SBP and DBP on similar lines (Table 3). The change in the nocturnal dip from baseline to day 56 for SBP and DBP was statistically nonsignificant in both groups. Moreover, the difference in mean change in the nocturnal dip for systolic and diastolic BP was statistically nonsignificant between the two treatment groups. The SI was obtained for SBP and DBP and was summarized for each treatment group, as shown in Table 4. The mean systolic and diastolic SI was higher in the telmisartan group as compared to the cilnidipine group; however, the difference was statistically nonsignificant. The number of responders in two treatment arms according to ABPM and manual measurements is shown in Figure 4. Both ABPM and manual measurements showed a higher number of responders in the telmisartan group than in the cilnidipine group, although the difference was statistically nonsignificant.
Click to view | Table 2. Descriptive Statistics for Various ABPM-Derived Variables and Their Comparison Within Groups as Well as Comparison of Change From Baseline to Day 56 Between Groups |
Click to view | Table 3. Descriptive Statistics for Nocturnal Dip and Its Comparison Within Group as Well as Comparison of Its Change From Baseline to Day 56 Between Two Groups |
Click to view | Table 4. Comparison of Smoothness Index Between Two Groups for Systolic and Diastolic BP |
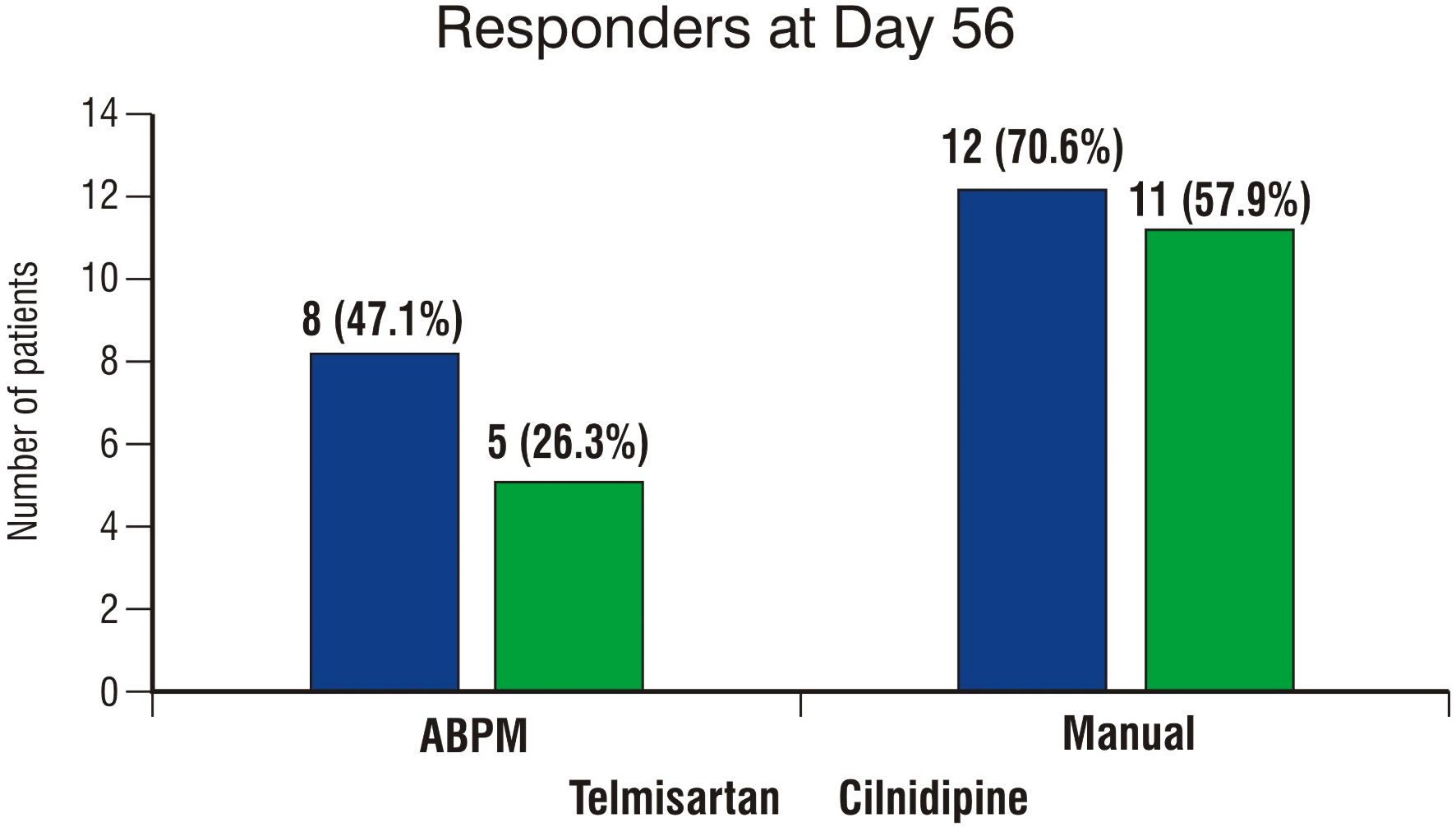 Click for large image | Figure 4. Column chart showing number of responders at day 56 in two groups for ABPM and manual BP measurement. ABPM: ambulatory blood pressure monitoring; BP: blood pressure. |
Regarding safety, none of the patients reported any AE during the course of the study. The lab parameters showed statistically nonsignificant differences within and between groups.
| Discussion | ▴Top |
The present study aimed at determining the efficacy and safety of telmisartan versus cilnidipine using an ABPM device. The ABPM approach provided a dynamic viewpoint of BP trends over 24 h in patients in these two treatment groups. The effectiveness of the treatment over different time durations could be explored through continuous monitoring, which was the value addition of the study as compared to manual office measurements. The overall profile of BP in both treatment groups was similar to that reported by Plavnik et al in 2002 [16]. In general, both hypertensive and normotensive individuals have similar circadian variation in BP, with higher values during the daytime and lower during the night times [17]. In the morning period, the BP surges; however, the extent of the surge varies with the individuals, and some even display morning hypertension [18]. In our study, we also observed a rise in the BP level in the morning session with a peak reaching at mid-day, then declining till evening and reaching lowest during night times. The pattern was consistent before and after medication; however, there was a significant reduction post-treatment in both groups.
Regarding the antihypertensive effect, the ABPM-derived variables exhibited better improvement in both SBP and DBP in the telmisartan group as compared to the cilnidipine-treated group. There was a significant within-group reduction in 24-h SBP and DBP in the telmisartan group, unlike in cilnidipine group, where only 24-h SBP was reduced significantly. Overall, the reduction was prominent in SBP as compared to DBP in both the groups. The last 6-h SBP and DBP showed significant improvement in the telmisartan group, unlike in the cilnidipine group. The difference of change in these parameters from baseline to day 56 was also significantly better with telmisartan as compared to cilnidipine. Earlier, telmisartan 40 mg or 80 mg demonstrated better control of both SBP and DBP during the last 6 h of dosing interval as compared to losartan 50 mg [19]. Telmisartan 40 mg showed a reduction of 10.7/6.8 mm Hg for SBP/DBP in patients, which was significant (P < 0.05). Our study showed a higher reduction of 16.77/10.76 mm Hg with the same dose. In PROBE study with telmisartan 80 mg and valsartan 80 mg, a significant reduction was seen in the last 6 h in DBP in the telmisartan-treated group after 8 weeks [20]. In PRISMA study, the authors observed superior reduction in SBP and DBP in the last 6 h with telmisartan 80 mg as compared to ramipril 10 mg after 14 weeks [21-23]. The evidence of telmisartan controlling the morning BP surge was also observed in MICCAT2 study [24]. Telmisartan 80 mg also proved to be more effective than ramipril 10 mg in reducing nighttime low and early morning mean SBP and DBP compared to baseline [25]. In our study, the nighttime improvement in SBP and DBP with telmisartan 40 mg was significantly better on day 56 as compared to baseline, while only SBP showed significant improvement with cilnidipine 10 mg. The reason for the superior effectiveness of telmisartan in the above studies could be that among all the ARBs, telmisartan has the longest half-life of about 24 h [26, 27]. This ensures its long duration of action and thereby effective control throughout the once-daily dose interval. Due to its lipophilic property, we observed a significant improvement in some of the ABPM-derived variables with cilnidipine; however, the effect was better with telmisartan than with cilnidipine.
The responder rate in the telmisartan group was higher (47.1%) than that in cilnidipine group (26.3%) based on ABPM data. The reported responder rate for ARBs ranges between 33-79%, while for calcium-channel blockers it ranges between 43-95% [28]. For telmisartan, the rate was within the reported range, while for cilnidipine, it was much below the observed rates. Another efficacy indicator nocturnal dip showed a higher percent increase for SBP and DBP in the telmisartan group than the cilnidipine group, although the change was statistically nonsignificant. Furthermore, the mean SI for SBP and DBP in the telmisartan group was higher than that in cilnidipine group for the study sample, although the difference in means was statistically nonsignificant. The higher index values in patients treated with telmisartan suggest better homogeneity or smoothing of BP reduction for the treatment [29]. There were no reported AEs during the study period in both the treatment groups and any deviations in laboratory parameters with respect to baseline values, thereby ensuring the safety of both the antihypertensive drugs. The smaller sample size is a limitation of the study, which may not allow generalization of the results to a larger population.
Conclusions
The efficacy and safety assessment of telmisartan 40 mg versus cilnidipine 10 mg using ABPM indicated the superiority of telmisartan over cilnidipine as regards last 6 h and morning time SBP as well as DBP. Telmisartan, with its longest half-life among ARBs, has the potential to reduce early morning BP, which has been demonstrated through numerous studies. Although cilnidipine showed improvement in the ABPM parameters, the effect was prominent in the telmisartan group. Both the drugs were well tolerated; however, considering the effective control of the morning BP surge, telmisartan can be a better choice for the management of mild to moderate hypertension.
Acknowledgments
We acknowledge the support provided by Ardent Clinical Research Pvt. Ltd., Pune, India for onsite clinical trial management.
Financial Disclosure
Investigator (Dr. Rahul Sawant) initiated the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
All the subjects provided written informed consent.
Author Contributions
Rahul Sawant was involved in conceptualization, study design and manuscript review. Sachin Suryawanshi and Hanmant Barkate reviewed and approved the manuscript. Mayur Jadhav and Sumit Bhushan performed statistical analysis, contributed to manuscript writing and proof reading. Tanmay Rane did final proof reading and approval for publication.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- World Health Organization (WHO). Fact Sheet on Non-communicable Diseases. 2021. Available from: https://www.who.int/news-room/factsheets/detail/noncommunicable-diseases. Access date: October 10, 2022.
- Whelton PK, Carey RM, Aronow WS, Casey DE, Jr., Collins KJ, Dennison Himmelfarb C, DePalma SM, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Hypertension. 2018;71(6):1269-1324.
doi pubmed - World Health Organization (WHO). Fact sheet on Hypertension. 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/hypertension. Access date: October 10, 2022.
- Shah SN, Munjal YP, Kamath SA, Wander GS, Mehta N, Mukherjee S, Kirpalani A, et al. Indian guidelines on hypertension-IV (2019). J Hum Hypertens. 2020;34(11):745-758.
doi pubmed - Bhatia M, Kumar M, Dixit P, Dwivedi LK. Diagnosis and Treatment of Hypertension Among People Aged 45 Years and Over in India: A Sub-national Analysis of the Variation in Performance of Indian States. Front Public Health. 2021;9:766458.
doi pubmed pmc - Dadlani A, Madan K, Sawhney JPS. Ambulatory blood pressure monitoring in clinical practice. Indian Heart J. 2019;71(1):91-97.
doi pubmed pmc - Grossman E. Ambulatory blood pressure monitoring in the diagnosis and management of hypertension. Diabetes Care. 2013;36(Suppl 2):S307-S311.
doi pubmed pmc - Gosse P. A review of telmisartan in the treatment of hypertension: blood pressure control in the early morning hours. Vasc Health Risk Manag. 2006;2(3):195-201.
doi pubmed pmc - Dolan E, Stanton A, Thijs L, Hinedi K, Atkins N, McClory S, Den Hond E, et al. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study. Hypertension. 2005;46(1):156-161.
doi pubmed - Wienen W, Entzeroth M, van Meel JCA, et al. A review on telmisartan: a novel, long-acting angiotensin II-receptor antagonist. Cardiovasc Drug Rev. 2000;18:127-156.
- Smith DH, Neutel JM, Lacourciere Y, Kempthorne-Rawson J. Prospective, randomized, open-label, blinded-endpoint (PROBE) designed trials yield the same results as double-blind, placebo-controlled trials with respect to ABPM measurements. J Hypertens. 2003;21(7):1291-1298.
doi pubmed - Grassi G. Sympathetic overdrive and cardiovascular risk in the metabolic syndrome. Hypertens Res. 2006;29(11):839-847.
doi pubmed - Takahara A. Cilnidipine: a new generation Ca channel blocker with inhibitory action on sympathetic neurotransmitter release. Cardiovasc Ther. 2009;27(2):124-139.
doi pubmed - Konda T, Enomoto A, Aritomi S, Niinuma K, Koganei H, Ogawa T, Nitta K. Different effects of L/N-type and L-type calcium channel blockers on the renin-angiotensin-aldosterone system in SHR/Izm. Am J Nephrol. 2009;30(2):155-161.
doi pubmed - Sharma S. Hypertension therapeutics update: a brief clinical summary of azilsartan, cilnidipine and nebivolol. Hypertens J. 2015;1(2):111-117.
- Plavnik FL, Riberio AB. A multicenter, open-label study of the efficacy and safety of telmisartan in mild to moderate hypertension patients. Arq Bras Card. 2002;79(4):345-350.
- Staessen JA, Bieniaszewski L, O'Brien E, Gosse P, Hayashi H, Imai Y, Kawasaki T, et al. Nocturnal blood pressure fall on ambulatory monitoring in a large international database. The “Ad Hoc” Working Group. Hypertension. 1997;29(1 Pt 1):30-39.
doi pubmed - Gosse P, Lasserre R, Minifie C, Lemetayer P, Clementy J. Blood pressure surge on rising. J Hypertens. 2004;22(6):1113-1118.
doi pubmed - Mallion J, Siche J, Lacourciere Y. ABPM comparison of the antihypertensive profiles of the selective angiotensin II receptor antagonists telmisartan and losartan in patients with mild-to-moderate hypertension. J Hum Hypertens. 1999;13(10):657-664.
doi pubmed - Littlejohn T, Mroczek W, Marbury T, VanderMaelen CP, Dubiel RF. A prospective, randomized, open-label trial comparing telmisartan 80 mg with valsartan 80 mg in patients with mild to moderate hypertension using ambulatory blood pressure monitoring. Can J Cardiol. 2000;16(9):1123-1132.
pubmed - Lacourciere Y, Neutel J, Koval SE, et al. A prospective, randomized investigation of the safety and efficacy of telmisartan vs ramipril in mild-to-moderate hypertensives using ambulatory blood pressure monitoring. Hypertension. 2004;44:576.
- Lacourciere Y, Neutel JM, Davidai G, Koval S. A multicenter, 14-week study of telmisartan and ramipril in patients with mild-to-moderate hypertension using ambulatory blood pressure monitoring. Am J Hypertens. 2006;19(1):104-112.
doi pubmed - Williams B, Gosse P, Lowe L, Harper R, PRISMA I Study Group. The prospective, randomized investigation of the safety and efficacy of telmisartan versus ramipril using ambulatory blood pressure monitoring (PRISMA I). J Hypertens. 2006;24(1):193-200.
doi pubmed - White WB, Weber MA, Davidai G, Neutel JM, Bakris GL, Giles T. Ambulatory blood pressure monitoring in the primary care setting: assessment of therapy on the circadian variation of blood pressure from the MICCAT-2 Trial. Blood Press Monit. 2005;10(3):157-163.
doi pubmed - Gosse P, Neutel JM, Schumacher H, et al. Reduction of early morning blood pressure surge with telmisartan compared with ramipril in mildto-moderate hypertensive patients. J Hypertens. 2005;23(2):S375-376.
- Burnier M, Maillard M. The comparative pharmacology of angiotensin II receptor antagonists. Blood Press Suppl. 2001;1:6-11.
pubmed - Brunner HR. The new oral angiotensin II antagonist olmesartan medoxomil: a concise overview. J Hum Hypertens. 2002;16 Suppl 2:S13-S16.
doi pubmed - Basile J. Blood pressure responder rates versus goal rates: which metric matters? Ther Adv Cardiovasc Dis. 2009;3(2):157-174.
doi pubmed - Parati G, Omboni S, Rizzoni D, Agabiti-Rosei E, Mancia G. The smoothness index: a new, reproducible and clinically relevant measure of the homogeneity of the blood pressure reduction with treatment for hypertension. J Hypertens. 1998;16(11):1685-1691.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.