

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 2, April 2023, pages 133-141

Nutritional Status in Patients Undergoing Phase II Cardiac Rehabilitation by Mini Nutritional Assessment
Yosuke Nozawaa, b, Miho Nishitani-Yokoyamaa, c, e, Kazunori Shimadaa, Hiroki Kasuyaa, Mitsuhiro Kunimotoa, Kei Fujiwaraa, Mayumi Doic, Yusei Satoc, Junya Nishimurac, Jianying Xua, Abidan Abulimitia, Minoru Tabatad, Tohru Minaminoa
aDepartment of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan
bMedical Affairs, Pfizer Japan Inc., Tokyo, Japan
cCardiovascular Rehabilitation and Fitness, Juntendo University Hospital, Tokyo, Japan
dDepartment of Cardiovascular Surgery, Juntendo University Graduate School of Juntendo Medicine, Tokyo, Japan
eCorresponding Author: Miho Nishitani-Yokoyama, Department of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, Bunkyo-ku, Tokyo 113-8421, Japan
Manuscript submitted February 1, 2023, accepted April 1, 2023, published online April 8, 2023
Short title: MNA in Cardiovascular Patients
doi: https://doi.org/10.14740/cr1479
| Abstract | ▴Top |
Background: Malnutrition impairs quality of life and prognosis of patients with cardiovascular disease. The Mini Nutritional Assessment (MNA) is a screening tool developed for the nutritional assessment of older adults. However, usefulness of MNA for patients undergoing cardiac rehabilitation (CR) has not been fully investigated.
Methods: From March 2017 to September 2019, the MNA-short form (MNA-SF) and the MNA total score in patients undergoing phase II CR at the Juntendo University Hospital were evaluated.
Results: A total of 336 patients (mean age 70.1 ± 11.4 years; males: 209) were analyzed. In the MNA-SF, 157 patients (47%) were found to be malnourished or at risk of malnutrition. In MNA total score, 168 patients (50%) were found to be malnourished or at risk of malnutrition. The MNA-SF < 12 group had significantly lower body mass index (BMI), hemoglobin level, low MNA scores for protein/water intake, self-evaluation of nutrition and health, and upper arm and calf circumferences compared to the MNA-SF ≥ 12 group. Assuming BMI < 18.5 as malnutrition, the sensitivity and specificity for malnutrition were 100% and 58.9% for MNA-SF, and 96.9% and 54.9% for MNA total score, respectively.
Conclusions: MNA is useful in screening for malnutrition in patients undergoing CR. Approximately 50% of them were determined to be malnourished or at risk of malnutrition, suggesting the need for detailed evaluation regarding their food intake and dietary intervention.
Keywords: Cardiac rehabilitation; Malnutrition; Mini Nutritional Assessment; Screening
| Introduction | ▴Top |
Cardiac rehabilitation (CR) is a comprehensive second prevention program that includes exercise therapy, coronary risk factor modification, disease management, and pharmacotherapy. This program aims to improve physical and psychological status and to reduce recurrence and death in patients with cardiovascular disease (CVD) [1]. A meta-analysis reported that CR is a cost-effective treatment that leads to significantly better quality-adjusted life-years than usual care in patients with coronary artery disease [2]. Recent studies have shown that frailty and sarcopenia caused by malnutrition or decreased activity in older adults are prognostic factors in heart failure patients [1, 3, 4]. To prevent the progression of frailty in patients with CVD, it is important to adopt comprehensive CR including appropriate nutritional and exercise therapy from early stage [5].
Malnutrition is highly prevalent in older adults undergoing rehabilitation [6, 7], and it is a risk factor for poor prognosis [8, 9]. The Mini Nutritional Assessment (MNA) is a widely used screening tool [10, 11] developed for the nutritional assessment of older adults [12, 13]. The MNA consists of six screening items and 12 assessment items, and the MNA total score is calculated from these 18 items [12, 13]. The six-item screening score, which is part of the MNA total score, is also used alone as the MNA-short form (MNA-SF) [14, 15]. Although there are several reports on the nutritional evaluation of patients undergoing CR using MNA-SF [14-16], there have been no reports on the MNA total score of Japanese patients undergoing CR. Therefore, we evaluated the nutritional status of CR patients using MNA-SF and MNA total score to examine the usefulness of them.
| Materials and Methods | ▴Top |
Subjects
This study recruited 356 patients undergoing phase II CR at Juntendo University Hospital from March 2017 to September 2019. This study included inpatients with stable cardiac function and those who had participated in early phase II CR.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and in compliance with the ethical guidelines for medical research involving human subjects. The protocol for this study was approved by the Ethics Committee of Juntendo University Hospital (17-307). Written consent to participate in the study was obtained from the participants.
Methods
This is a retrospective study that evaluated nutritional status using MNA in patients undergoing CR. In this study, we assumed that body mass index (BMI) < 18.5 as malnutrition [1], and we evaluated: 1) correlation between MNA-SF and MNA total score and BMI; 2) the screening accuracy of MNA-SF and MNA total score for malnutrition; 3) patient characteristics between MNA-SF categories; and 4) equivalence of MNA-SF for MNA total score. BMI was measured using a body composition analyzer (TANITA, MC 780A, Tokyo, Japan) at the beginning of CR in hospitalized patients with stable cardiac function. Study flow is shown in Figure 1. To evaluate the screening accuracy for malnutrition, the area under the curve (AUC) in the receiver operating characteristic (ROC) analysis and the sensitivity and specificity for the MNA-SF with a cut-off value of 12 and the MNA total score with a cut-off value of 24 were calculated. Patient characteristics, score of each item of MNA and results of MNA-SF and MNA total score were compared between the MNA-SF categories. We calculated the sensitivity and specificity of the MNA-SF category for the MNA total score category. The cut-off value of the MNA-SF score for the MNA total score category was calculated from the actual data in this study. In addition, patient background was analyzed for those whose MNA-SF and MNA total score judgment were inconsistent.
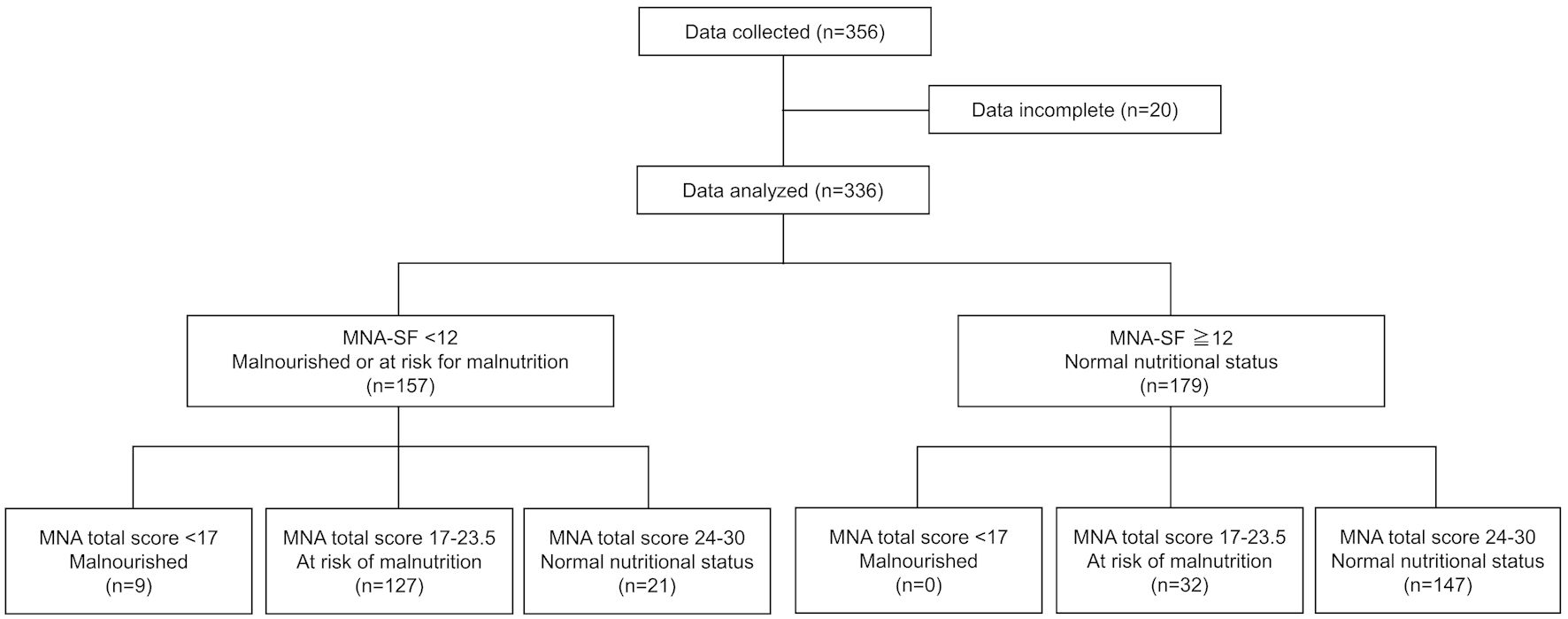 Click for large image | Figure 1. Study flow. CR: cardiac rehabilitation, MNA: Mini Nutritional Assessment; SF: short form. |
MNA
The MNA total score consists of 18 items as follows (maximum score 30): 1) food intake; 2) weight loss; 3) mobility; 4) psychological stress; 5) neuropsychological problems; 6) BMI; 7) living independently; 8) number of medications; 9) skin ulcers; 10) number of meals; 11) protein intake; 12) fruit or vegetables intake; 13) fluid intake; 14) mode of feeding; 15) self-assessment of nutritional status; 16) self-assessment of health status; 17) mid-arm circumference; and 18) calf circumference [12, 13]. MNA-SF is scored on items 1) to 6) (maximum score 14). For MNA-SF, 12 - 14 points indicate a normal nutritional status, 8 - 11 points indicate at risk of malnutrition, and 7 points or less indicate malnourishment, whereas for MNA total score, these are attributed to 24 - 30, 17 - 23.5, and < 17 points, respectively. The MNA total score is usually calculated for patients with MNA-SF score < 12 [12, 13]; however, in this study, the MNA total score was calculated for all patients. The MNA-SF and MNA total score were evaluated at the beginning of phase II CR.
Blood biochemistry test
The estimated glomerular filtration rate was calculated based on serum creatinine (Cre), sex, and age [17]. Blood biochemical tests were conducted for serum hemoglobin (Hb), Cre, low-density lipoprotein cholesterol, triglycerides, high-density protein cholesterol, hemoglobin A1c (HbA1c), and C-reactive protein (CRP) at the beginning of CR.
Statistical analysis
Descriptive statistics were expressed as n (%) and mean ± standard deviation (SD). The Spearman’s rank correlation coefficient was used to evaluate the correlation between MNA-SF and MNA total score and BMI. The χ2 test was used to compare categorical variables, and the Wilcoxon rank sum test was used to compare continuous variables. The significance level was set to < 0.05 on both sides. The cut-off values of MNA-SF for MNA total score categories and AUC of ROC curve were calculated in a ROC analysis. Sensitivity and specificity were calculated for the accuracy of judgment for various cut-off values. Statistical analysis was performed using JMP ver. 16.2.0 (SAS Institute Inc., Cary, NC, USA).
| Results | ▴Top |
Patient characteristics
In a total of 356 patients, 20 patients were excluded because of incomplete data; therefore, 336 patients were included in the analysis (Fig. 1). The age of the patients was 70.1 ± 11.4 years, and 209 (62.2%) of them were male (Table 1). CVD at beginning of CR were post-open-heart surgery for 151 patients (44.9%), chronic heart failure for 119 patients (35.4%), and other for 66 patients (19.6%). Acute coronary syndrome (ACS) was present in 33 patients (9.8%). There were 157 and 179 patients in the MNA-SF < 12 group and MNA-SF ≥ 12 group, respectively. The proportion of ACS was relatively higher in the MNA-SF < 12 group compared to the MNA-SF ≥ 12 group (12.1% vs. 7.8%), but there was no significant difference between the groups. BMI and Hb levels were significantly lower in the MNA-SF < 12 group than in the ≥ 12 group, but there were no significant differences in other patient characteristics.
 Click to view | Table 1. Patient Characteristics |
MNA
The results of MNA-SF and MNA total score are shown in Table 2. In all patients, MNA-SF showed 21 patients (6.3%) of malnourished, 136 patients (40.5%) of at risk of malnutrition, and 179 patients (53.3%) of normal nutritional status, with the MNA total score of nine (2.7%), 159 (47.3%) and 168 (50.0%), respectively. Of the 157 patients with MNA-SF < 12, nine patients (5.7%) were malnourished, 127 patients (80.9%) were at risk of malnutrition, and 21 patients (13.4%) were normal nutritional status according to the MNA total score. Similarly, in 179 patients with MNA-SF ≥ 12, malnourished was not observed, 32 patients (17.9%) were at risk of malnutrition, and 147 patients (82.1%) were normal nutritional status by the MNA total score. Compared to the MNA-SF ≥ 12 group, the MNA-SF < 12 group presented significantly lower scores on the MNA assessment for protein intake, water intake, self-assessment of nutritional and health status, upper arm circumference, and calf circumference.
Click to view | Table 2. MNA Results |
Screening accuracy of MNA-SF and MNA total score for malnutrition
Correlations between MNA-SF and MNA total score and BMI are shown in Figure 2. Both MNA-SF and MNA total score were significantly positively correlated with BMI (r = 0.446, P < 0.001 and r = 0.496, P < 0.001, respectively). ROC analysis showed that AUC of MNA-SF for malnutrition (BMI < 18.5) was 0.811, and the sensitivity of MNA-SF with cut-off value of 12 for malnutrition was 100.0%, with a specificity of 58.9% (Fig. 3a). Similarly, AUC of MNA total score for malnutrition was 0.838, and the sensitivity and specificity of the MNA total score with cut-off value of 24 were 96.9% and 54.9%, respectively (Fig. 3b).
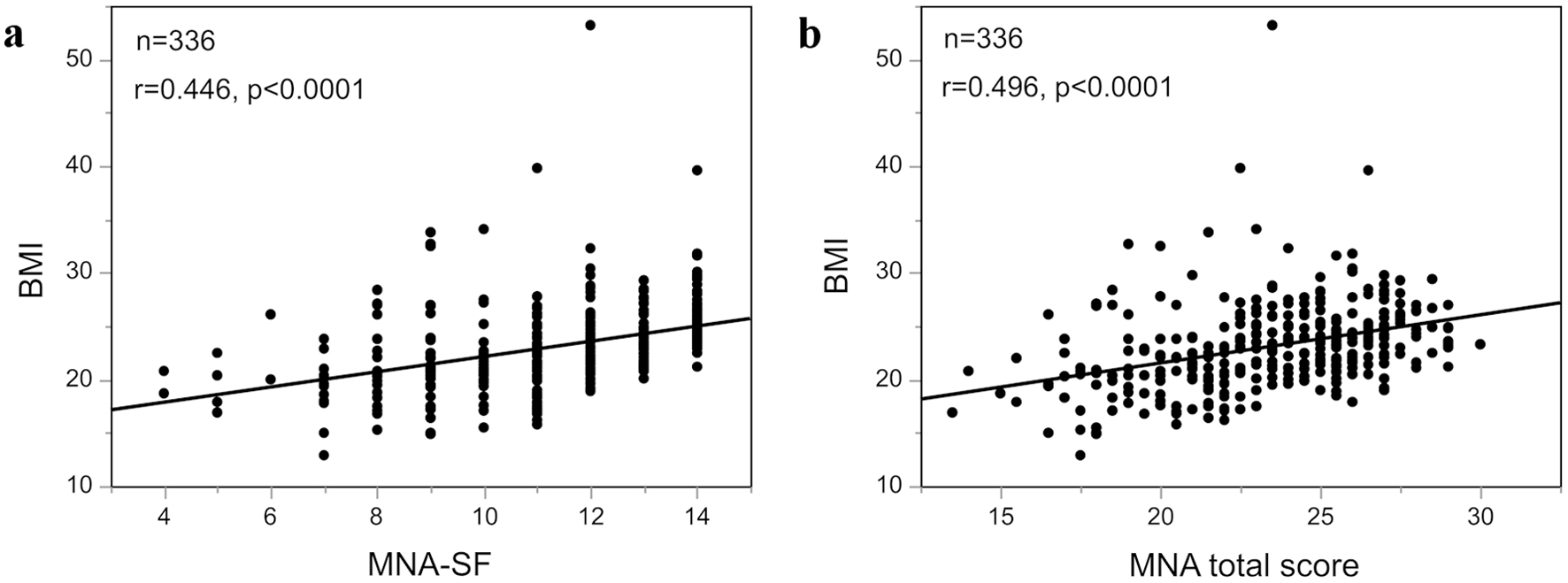 Click for large image | Figure 2. Correlation between MNA-SF and MNA total score and BMI. (a) Correlation between MNA-SF and BMI. (b) Correlation between MNA total score and BMI. MNA: Mini Nutritional Assessment; SF: short form; BMI: body mass index. |
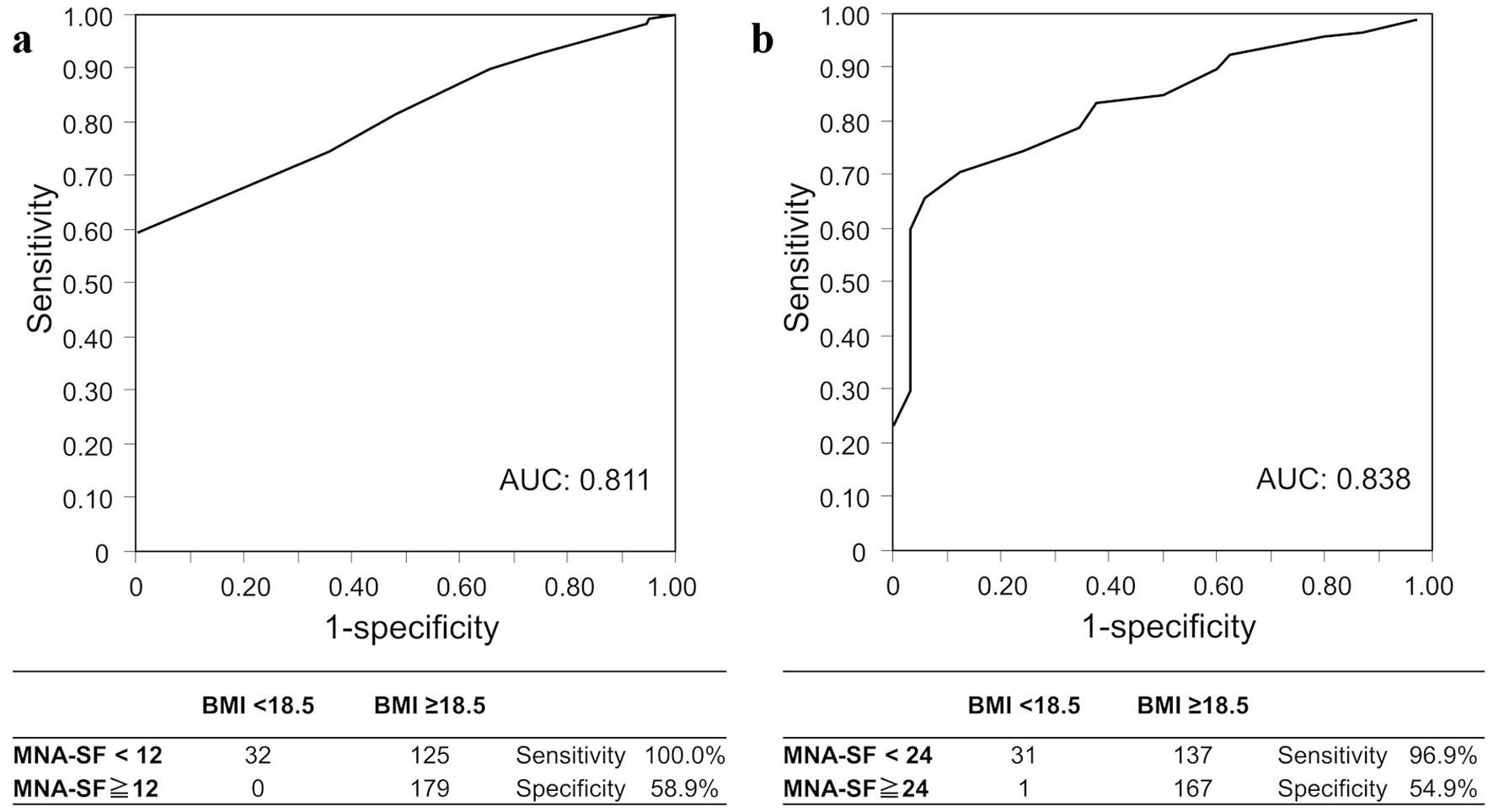 Click for large image | Figure 3. Screening accuracy of (a) MNA-SF and (b) MNA total score for malnutrition. AUC: area under the curve; MNA: mini nutritional assessment; ROC: receiver operator characteristic; SF: short form. |
Validity of cut-off values for MNA-SF
The ROC analysis of the MNA-SF score for the MNA total score < 24 (malnourished or at risk of malnutrition) indicated that AUC was 0.904 and the cutoff of MNA-SF score was 12, which was consistent with the commonly used cut-off value (Fig. 4). The MNA-SF with cut-off value of 12 presented a sensitivity of 81.0% and specificity of 87.5% for the MNA total score < 24 (Fig. 4).
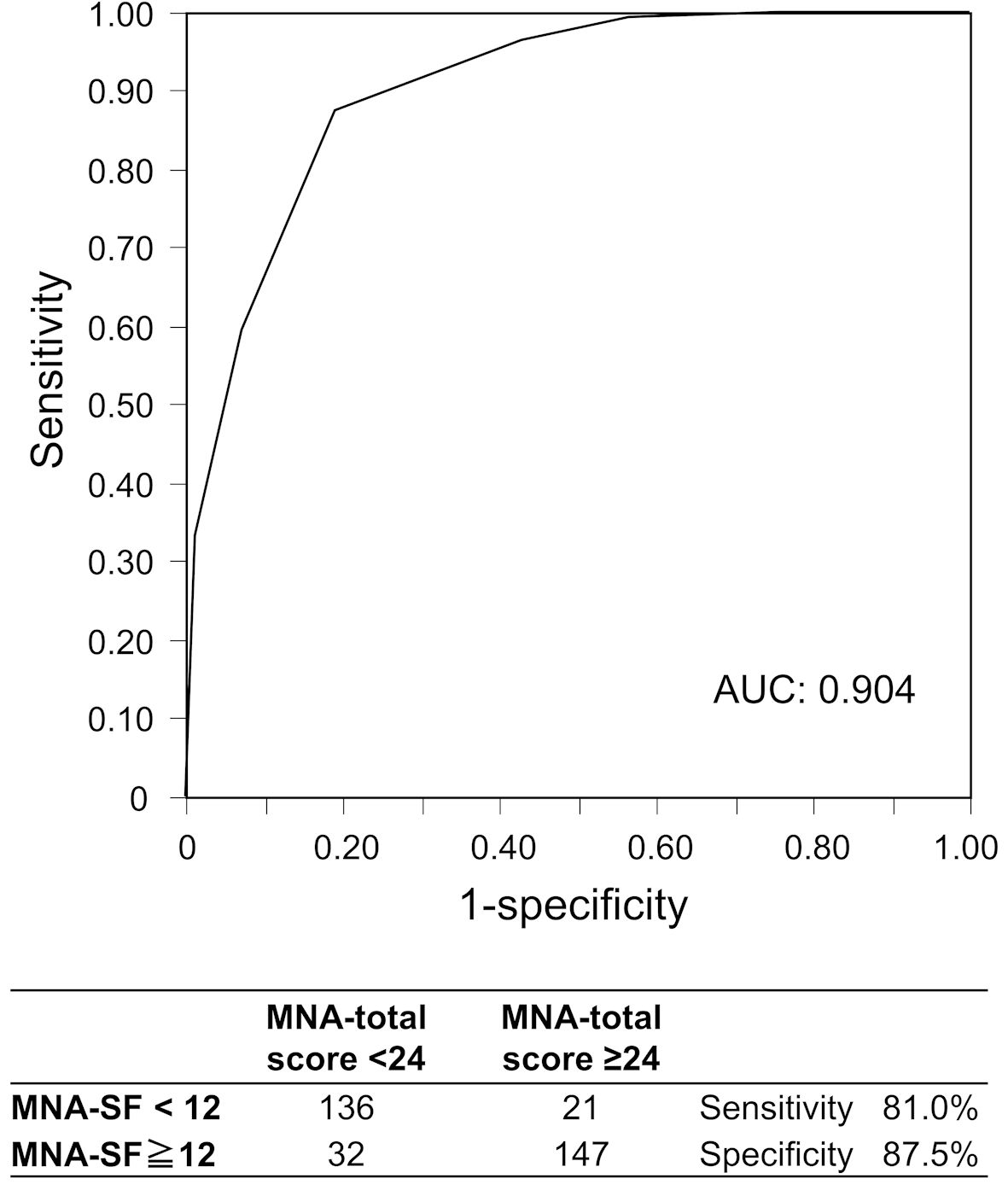 Click for large image | Figure 4. ROC curves of MNA-SF for MNA overall score < 24. AUC: area under the curve; MNA: Mini Nutritional Assessment; ROC: receiver operator characteristic; SF: short form. |
Discrepancies between MNA-SF and MNA total score
The MNA-SF < 12 group included 21 patients (13.4%) with MNA total score ≥ 24, whereas the MNA-SF ≥ 12 group included 32 patients (17.9%) with MNA total score < 24 (Table 3). In the MNA-SF < 12 group, compared to the patients with MNA total score < 24, patients with MNA total score ≥ 24 presented significantly higher male proportion and Hb levels and significantly lower CRP levels, with no significant differences in other parameters. In the MNA-SF ≥ 12 group, compared to patients with MNA total score ≥ 24, patients with MNA total score < 24 presented significantly lower BMI, and there were no significant differences in other parameters.
Click to view | Table 3. Background Characteristics of Patients With Discrepancies Between MNA-SF and MNA Total Score |
| Discussion | ▴Top |
The nutritional status of 336 patients undergoing CR was evaluated by the MNA. The number of patients classified as malnourished or at risk of malnutrition according to the MNA-SF and MNA total score was 157 (46.7%), and 168 (50.0%), respectively. Sensitivity and specificity for malnutrition were 100% and 58.9% for MNA-SF, and 96.9% and 54.9% for MNA total score, respectively. In addition, the sensitivity and specificity of the MNA-SF for MNA total score < 24 were 81.0% and 87.5%, respectively, suggesting that both MNA-SF and MNA total scores are useful for the nutritional assessment of patients undergoing CR. Compared to the MNA-SF ≥ 12 group, the MNA-SF < 12 group presented significantly lower BMI and Hb and significantly lower scores on the MNA assessment for protein and water intake and self-assessment of nutritional and health status, which indicated the need for dietary intervention. This is the first report evaluating the usefulness of the MNA total score for Japanese CR patients.
In our study, in patients with a mean age of 70.1 years, the MNA-SF indicated 6.3%, 40.5%, and 53.3% of malnourished, at risk of malnutrition, and normal nutritional status, whereas MNA total score indicated 2.7%, 47.3%, and 50.0%, respectively. Fukui et al reported that an MNA-SF in older adults with aortic stenosis in Japan with a mean age of 83.8 years indicated 11.3% of malnourished, 42.3% of at risk of malnutrition, and 46.4% of normal [18]. Considering the difference in mean age of patients, our results appeared to be similar to those reported by Fukui et al [18]. On the other hand, regarding reports from other countries, in Germany, Kather et al evaluated MNA-SF in older adults undergoing CR with a mean age of 82.3 years, with 4.9% malnourished, 33.6% at risk for malnutrition, and 61.5% normal [14]. In Italy, Tonet et al evaluated MNA-SF in ACS patients with a mean age of 82 years, with 4% malnourished, 40% at risk for malnutrition, and 56% normal [19]. In Italy, Passantino et al evaluated the MNA total score in CR patients with a mean age of 67.1 years, with 1.9% malnourished, 40.1% risk of malnutrition, and 58% normal [20]. Our results on the distribution of nutritional status were comparable to those reported in the Europe.
In this study, BMI < 18.5 was used as an indicator of malnutrition. BMI is not an absolute indicator of malnutrition, but it is one of indicator to assess malnutrition. We compared the accuracy of the MNA-SF and MNA total score for malnutrition under the same conditions, with a cut-off value for BMI assuming malnutrition. We think the issue to be cleared is the accuracy of using BMI to determine malnutrition. In the Global Leadership Initiative on Malnutrition (GLIM) report of 2019, low BMI was a diagnostic criterium for malnutrition [21-23], and reference values included BMI < 18.5 for Asians of < 70 years and BMI < 20 for those of ≥ 70 years [1]. In addition, Zhang et al reported a meta-analysis of various indicators for determining malnutrition in the older adults [24]. In their report, BMI was a significant determinant for all malnutrition status defined by MNA < 17, Subjective Global Assessment (SGA) of C, Nutrition Risk Screening 2002 ≥ 3, and Geriatric Nutritional Risk Index < 92, with cut-off values (95% CI) of 20.89 (19.81, 21.96), 19.77 (18.11, 231.42) 22.60 (21.23, 23.97) and 20.24 (18.46, 22.03), respectively [24]. Given these results, we believe that the BMI cut-off value we used (< 18.5) was reasonable in assuming malnutrition.
The sensitivity and specificity of MNA-SF with a cut-off value of 12 for malnutrition were 100.0% and 58.9%, whereas those of MNA total score with cut-off value of 24 were 96.9% and 54.9%, respectively. In this study, the sensitivity of both MNA-SF and MNA total score to malnutrition was sufficiently high, and both seemed to be effective for malnutrition screening.
AUC of ROC curve for malnutrition was slightly higher in MNA total score than MNA-SF (0.837 vs. 0.811). The sensitivity and specificity of the MNA-SF with cut-off value of 12 for the MNA total score < 24 were 81.0%, and 87.5%, respectively. The cut-off value of MNA-SF for the MNA total score < 24 in the ROC analysis according to the actual data of this study was 12, which is consistent with the commonly used cut-off value of MNA-SF. These results suggest that the current cut-off value of MNA-SF is also reasonable for CR patients in Japan.
On the other hand, the 81.0% of sensitivity of MNA-SF to MNA total score < 24 indicates that 19% of patients with MNA total score < 24 will be missed by MNA-SF. The MNA-SF < 12 group included 12.5% of patients with MNA total score ≥ 24, and the MNA-SF ≥ 12 group included 20.1% of patients with MNA total score < 24. These results indicate that there was some discrepancy between MNA-SF and MNA total score. For MNA-SF < 12 patients, MNA total score will be evaluated in clinical practice, thus cases with MNA-SF ≥ 12 and MNA total score < 24 were clinically problematic. In patients with MNA-SF ≥ 12, those with an MNA total score < 24 presented a significantly lower BMI compared to those with MNA total score ≥ 24. Therefore, to reduce the risk of missing out on malnutrition, evaluation of MNA total score should be considered in cases with low BMI even with MNA-SF ≥ 12. The BMI cut-off value corresponding to MNA total score < 24 was calculated as 21.1 (AUC: 0.717) in the ROC analysis (data not shown). Therefore, even if MNA-SF ≥ 12, the MNA total score should be evaluated for cases with BMI ≤ 22.
In our study, the MNA-SF < 12 group showed significantly lower protein and water intake than the MNA-SF ≥ 12 group. Amino acid intake can enhance the effects of exercise in older women with sarcopenia [3]. Moreover, amino acid intake in older adults with frailty or pre-frailty can improve the lower limb muscle strength and physical function [25]. Therefore, it is important to evaluate the nutritional status and nutritional guidance including detail intake to improve physical function and quality of life.
The present study had several limitations. This was a single-center study; therefore, the results might contain selection bias. For instance, 92.0% of patients could walk freely outside, 97.3% had no mental problems, and 96.7% could eat on their own (data not shown). The study included only patients who had stable cardiac function and had participated CR. In this study, BMI < 18.5 was used as a malnutrition indicator. BMI can be affected by cognitive function, heart failure status, fluid retention and dietary intake. In addition, this study did not assess malnutrition by GLIM or SGA. Time from hospitalization or surgery to initiation of CR was not considered. The MNA sensitivity to malnutrition might vary if other indicators are used. Therefore, the results of this study should be interpreted with these considerations in mind.
Conclusions
MNA-SF and MNA total score are useful for evaluating the nutritional status of patients undergoing CR, and the current cut-off values for MNA-SF and MNA total score are appropriate for patients undergoing CR. Approximately half of phase II CR patients might be malnourished or at risk of malnutrition, which suggests the need for nutritional intervention including nutritional guidance.
Acknowledgments
The authors would like to thank all study participants and the collaborators who collected data on cardiovascular rehabilitation and fitness. Akio Honzawa and Yuki Someya have assisted and supported in sample collection.
Financial Disclosure
The authors declare that there is no funding for this research.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Informed Consent
Informed consent was obtained.
Author Contributions
YN has designed and performed the study. YN, MN-Y, KS and TM have drafted and edited the manuscript. MD, YS, JN, MK, KF, HK, JX, AA, and MT have assisted data collection. YN supervised the writing of this manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
AUC: area under the curve; BMI: body mass index; CR: cardiac rehabilitation; CRP: C-reactive protein; CVD: cardiovascular disease; GLIM: Global Leadership Initiative on Malnutrition; Hb: hemoglobin; MNA: Mini Nutritional Assessment; MNA-SF: Mini Nutritional Assessment-short form; ROC: receiver operating characteristic
| References | ▴Top |
- Makita S, Yasu T, Akashi YJ, Adachi H, Izawa H, Ishihara S, Iso Y, et al. JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease. Circ J. 2022;87(1):155-235.
doi
pmc - Takura T, Ebata-Kogure N, Goto Y, Kohzuki M, Nagayama M, Oikawa K, Koyama T, et al. Cost-effectiveness of cardiac rehabilitation in patients with coronary artery disease: a meta-analysis. Cardiol Res Pract. 2019;2019:1840894.
doi pubmed pmc - Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyere O, Cederholm T, Cooper C, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(4):601.
doi pubmed pmc - Roberts S, Collins P, Rattray M. Identifying and managing malnutrition, frailty and sarcopenia in the community: a narrative review. Nutrients. 2021;13(7):2316.
doi pubmed pmc - Ueno K, Kaneko H, Itoh H, Takeda N, Morita H, Fujiu K, Kamiya K, et al. Effectiveness and approach of rehabilitation in patients with acute heart failure: a review. Korean Circ J. 2022;52(8):576-592.
doi pubmed pmc - Shimizu A, Fujishima I, Maeda K, Murotani K, Inoue T, Ohno T, Nomoto A, et al. Accuracy of the simplified nutritional appetite questionnaire for malnutrition and sarcopenia screening among older patients requiring rehabilitation. Nutrients. 2021;13(8):2738.
doi pubmed pmc - Nishioka S, Matsushita T, Yamanouchi A, Okazaki Y, Oishi K, Nishioka E, Mori N, et al. Prevalence and associated factors of coexistence of malnutrition and sarcopenia in geriatric rehabilitation. Nutrients. 2021;13(11):3745.
doi pubmed pmc - Davis JP, Wong AA, Schluter PJ, Henderson RD, O'Sullivan JD, Read SJ. Impact of premorbid undernutrition on outcome in stroke patients. Stroke. 2004;35(8):1930-1934.
doi
pmc - Tsuji S, Koyama S, Taniguchi R, Fujiwara T, Fujiwara H, Sato Y. Association of serum amino acid concentration with loss of skeletal muscle mass after 1 year in cardiac rehabilitation center patients. Circ Rep. 2019;1(10):456-461.
doi pubmed pmc - Kuzuya M, Kanda S, Koike T, Suzuki Y, Satake S, Iguchi A. Evaluation of Mini-Nutritional Assessment for Japanese frail elderly. Nutrition. 2005;21(4):498-503.
doi
pmc - Elkan AC, Engvall IL, Cederholm T, Hafstrom I. Rheumatoid cachexia, central obesity and malnutrition in patients with low-active rheumatoid arthritis: feasibility of anthropometry, Mini Nutritional Assessment and body composition techniques. Eur J Nutr. 2009;48(5):315-322.
doi
pmc - Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, Albarede JL. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. 1999;15(2):116-122.
doi
pmc - Guigoz Y, Lauque S, Vellas BJ. Identifying the elderly at risk for malnutrition. The mini nutritional assessment. Clin Geriatr Med. 2002;18(4):737-757.
doi
pmc - Kather F, Hadzic M, Hehle T, Eichler S, Klein J, Voller H, Salzwedel A. Test-retest reliability of the Mini Nutritional Assessment-Short Form (MNA-SF) in older patients undergoing cardiac rehabilitation. J Geriatr Cardiol. 2020;17(9):574-579.
doi pubmed pmc - Wakabayashi H, Sashika H. Malnutrition is associated with poor rehabilitation outcome in elderly inpatients with hospital-associated deconditioning a prospective cohort study. J Rehabil Med. 2014;46(3):277-282.
doi
pmc - Katano S, Hashimoto A, Ohori K, Watanabe A, Honma R, Yanase R, Ishigo T, et al. Nutritional status and energy intake as predictors of functional status after cardiac rehabilitation in elderly inpatients with heart failure - a retrospective cohort study. Circ J. 2018;82(6):1584-1591.
doi
pmc - Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53(6):982-992.
doi
pmc - Fukui S, Kawakami M, Otaka Y, Ishikawa A, Muraoka K, Yashima F, Hayashida K, et al. Malnutrition among elderly patients with severe aortic stenosis. Aging Clin Exp Res. 2020;32(3):373-379.
doi
pmc - Tonet E, Campo G, Maietti E, Formiga F, Martinez-Selles M, Pavasini R, Biscaglia S, et al. Nutritional status and all-cause mortality in older adults with acute coronary syndrome. Clin Nutr. 2020;39(5):1572-1579.
doi
pmc - Passantino A, Guida P, Rizzo C, Carbonara R, Ruggieri R, Scrutinio D. Malnutrition in patients admitted to in-hospital cardiac rehabilitation: Clinical correlates and association with mortality. Monaldi Arch Chest Dis. 2021;92(2):1960.
doi
pmc - Cederholm T, Jensen GL, Correia M, Gonzalez MC, Fukushima R, Higashiguchi T, Baptista G, et al. GLIM criteria for the diagnosis of malnutrition - A consensus report from the global clinical nutrition community. Clin Nutr. 2019;38(1):1-9.
doi
pmc - de van der Schueren MAE, Keller H, Consortium G, Cederholm T, Barazzoni R, Compher C, Correia M, et al. Global Leadership Initiative on Malnutrition (GLIM): Guidance on validation of the operational criteria for the diagnosis of protein-energy malnutrition in adults. Clin Nutr. 2020;39(9):2872-2880.
doi
pmc - Norman K, Hass U, Pirlich M. Malnutrition in older adults-recent advances and remaining challenges. Nutrients. 2021;13(8):2764.
doi pubmed pmc - Zhang Z, Pereira SL, Luo M, Matheson EM. Evaluation of blood biomarkers associated with risk of malnutrition in older adults: a systematic review and meta-analysis. Nutrients. 2017;9(8):829.
doi pubmed pmc - Ikeda T, Aizawa J, Nagasawa H, Gomi I, Kugota H, Nanjo K, Jinno T, et al. Effects and feasibility of exercise therapy combined with branched-chain amino acid supplementation on muscle strengthening in frail and pre-frail elderly people requiring long-term care: a crossover trial. Appl Physiol Nutr Metab. 2016;41(4):438-445.
doi
pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.