

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 3, June 2024, pages 153-168

Comparative Efficacy of Percutaneous Coronary Intervention Versus Coronary Artery Bypass Grafting in the Treatment of Ischemic Heart Disease: A Systematic Review and Meta-Analysis of Recent Randomized Controlled Trials
Jordan Llerena-Velasteguia, b, h ![]() , Kristina Zumbana-Podanevaa
, Kristina Zumbana-Podanevaa ![]() , Sebastian Velastegui-Zuritaa
, Sebastian Velastegui-Zuritaa ![]() , Melany Mejia-Moraa
, Melany Mejia-Moraa ![]() , Juan Perez-Tomassettic, Allison Cabrera-Cruzd
, Juan Perez-Tomassettic, Allison Cabrera-Cruzd ![]() , Pablo Haro-Arteagae
, Pablo Haro-Arteagae ![]() , Ana Clara Fonseca Souza de Jesusf
, Ana Clara Fonseca Souza de Jesusf ![]() , Pedro Moraes Coelhof
, Pedro Moraes Coelhof ![]() , Cristian Sanahuja-Montielg
, Cristian Sanahuja-Montielg ![]()
aPontifical Catholic University of Ecuador, Medical School, Quito, Ecuador
bCenter for Health Research in Latin America (CISeAL), Research Center, Quito, Ecuador
cUniversity of the Americas, Medical School, Quito, Ecuador
dCatholic University of Santiago de Guayaquil, Medical School, Guayaquil, Ecuador
eUniversity of La Rioja, Logrono, Spain
fFaculdade de Minas - FAMINAS-BH, Medical School, Belo Horizonte, Brazil
gUniversity of Medical Sciences, Medical School, San Jose, Costa Rica
hCorresponding Author: Jordan Llerena-Velastegui, Pontifical Catholic University of Ecuador, Medical School, Quito, Ecuador
Manuscript submitted March 18, 2024, accepted April 27, 2024, published online June 25, 2024
Short title: PCI Versus CABG in Treatment of IHD
doi: https://doi.org/10.14740/cr1638
| Abstract | ▴Top |
Background: Ischemic heart disease (IHD) is a major global health issue and a leading cause of death. This study compares the effectiveness of percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) in the management of IHD, focusing on their impact on revascularization, myocardial infarction (MI), and post-procedural stroke. This study aimed to evaluate and compare the effectiveness of PCI and CABG in treating IHD based on an exhaustive literature review of the past 5 years, emphasizing recent advancements and outcomes in IHD management.
Methods: A comprehensive literature review analyzed 32 randomized controlled trials (RCTs) retrieved from databases such as PubMed, Cochrane Library, and Google Scholar. The study specifically assessed the incidences of revascularization, stroke, and MI in patients treated with either PCI or CABG. The comparison between CABG and PCI exclusively focused on lesions with a SYNTAX score exceeding 32.
Results: Our findings highlight CABG’s significant efficacy over PCI in reducing revascularization and MI. The aggregated Mantel-Haenszel (M-H) value for revascularization was 1.85 (95% confidence interval (CI): 1.65 - 2.07), signifying CABG’s advantage. Additionally, CABG demonstrated superior performance in diminishing MI occurrences (M-H = 2.71, 95% CI: 1.13 - 6.53). In contrast, PCI was more effective in reducing stroke (M-H = 0.80, 95% CI: 0.60 - 1.10).
Conclusion: The study confirms CABG’s superiority in reducing revascularization and MI in IHD patients, highlighting PCI’s effectiveness in reducing stroke risk. These findings underscore the importance of personalized treatment strategies in IHD management and emphasize the need for ongoing research and evidence-based guidelines to aid in treatment selection for IHD patients.
Keywords: Ischemic heart disease; Revascularization; Percutaneous coronary intervention; Coronary artery bypass graft surgery; Meta-analysis
| Introduction | ▴Top |
Recent epidemiological data reveal that ischemic heart disease (IHD) affects approximately 126 million individuals globally, accounting for about 1.72% of the world’s population (1,655 cases per 100,000 people) [1]. As a leading cause of death worldwide, IHD significantly contributes to the global disease burden, responsible for 7,249,000 deaths (12.7% of total global mortality) in 2008 [2]. IHD, also known as coronary artery disease (CAD), is characterized by reduced blood supply to the heart muscles, primarily due to the formation of plaque within coronary arteries. This condition may also be exacerbated by vessel narrowing and thrombus formation [3, 4].
The management of IHD involves a range of treatment options, from guideline-directed medical therapy (GDMT) to various surgical interventions. Myocardial revascularization, a key treatment strategy, has been shown to significantly enhance patient prognosis and survival rates [5]. This revascularization can be achieved through percutaneous coronary intervention (PCI) or coronary artery bypass graft surgery (CABG). PCI, particularly with the advent of the latest drug-eluting stents, calcium modification technologies, and advanced intravascular imaging, has evolved rapidly as a primary revascularization method for patients with severe coronary disease [6, 7]. On the other hand, CABG, an open-heart surgery technique, involves grafting a section of a blood vessel from the aorta to the coronary artery to bypass the ischemic region and improve blood supply [8]. Notably, the likelihood of undergoing CABG increases with age due to the progression of cardiovascular health issues [9].
The choice of revascularization method is influenced by a combination of patient preference, cardiac and extracardiac characteristics, and the complexity of coronary vessels, which is often assessed using the SYNTAX score. For patients with a low SYNTAX score (≤ 22), both PCI and CABG are recommended equally. However, CABG is advised over PCI for those with an intermediate SYNTAX score (23 - 32). In cases of highly complex coronary architecture (SYNTAX score ≥ 33), CABG is the only recommended option, with PCI not advised due to increased risks [10]. This tailored approach to treatment selection underscores the need for a personalized strategy in managing IHD, catering to the specific needs and conditions of individual patients.
Rationale
While existing literature has explored various interventions for IHD, there remains a scarcity of detailed statistical analysis specifically comparing the efficacies of PCI and CABG. Previous systematic reviews and meta-analyses have primarily focused on mortality rates and their contributing factors as the central point of efficacy comparison. This study aims to fill this gap by re-evaluating and providing a more nuanced understanding of the efficacy of these treatments. The primary endpoint for this analysis is the incidence of revascularization in both PCI and CABG. Additionally, we aim to assess the incidence of post-procedural complications, specifically stroke and myocardial infarction (MI), as critical secondary endpoints. This approach offers a more comprehensive evaluation of these interventions, contributing to a deeper understanding of their roles in IHD management.
Objectives
The primary aims of this study are threefold: 1) to critically assess and compare the efficacy of PCI and CABG specifically in the realm of revascularization for patients with IHD; 2) to examine patient outcomes, particularly focusing on the cumulative incidence of critical cardiovascular events, including MI and stroke (SE); and 3) to generate enhanced insights and develop evidence-based recommendations that will guide cardiothoracic surgeons and medical practitioners in selecting the most suitable treatment modality for IHD, thereby improving patient care and outcomes.
This review has been successfully registered in the international database PROSPERO under the ID CRD42024524618.
Definition
SYNTAX score
The SYNTAX score is an angiographic tool used by cardiologists, interventionists, and surgeons to assess the degree of complexity in coronary artery lesions. It helps inform individualized treatment decisions and provides prognostic data based on the anatomical disease burden of the heart [11].
Revascularization
Procedures that restore blood flow to the heart muscle are commonly referred to as revascularization in IHD. These may include procedures like PCI with stent implantation or CABG. Revascularization is intended to treat individuals with impaired cardiac blood flow to relieve symptoms, improve heart health, and reduce the risk of adverse outcomes [12].
Kaplan-Meier (KM) score
The KM survival curve is defined as the probability of surviving in a given length of time while considering time in many small intervals [13].
MI
MI is a term used for an event of heart attack, which is related to the formation of plaques in the inside walls of the arteries, resulting in reduced blood flow to the heart and affecting cardiac muscles due to a lack of oxygen supply [14].
Stroke
Acute, focal neurological impairment that is clinically diagnosed as a stroke is caused by vascular injury (hemorrhage, infarction) to the central nervous system. Stroke is the second most common cause of death and disability globally [15].
Efficacy
The ability of a particular intervention, such as medication, medical device, surgical technique, or public health activity, to produce a positive change (or therapeutic effect) in optimal or controlled settings is known as efficacy [16].
PCI
PCI is the most commonly used method for improving myocardial perfusion when treating CAD. A stent is inserted to scaffold the vessel after a balloon is used to dilate the coronary stenosis [17].
CABG
CABG uses arterial grafts and is more durable than PCI. It remains the gold standard for extensive CAD, involving three vessels or the left main stem [18].
IHD
IHD results from a limited blood supply to the heart muscle. IHD is commonly referred to as “coronary heart disease”, since coronary blood flow loss brought on by coronary artery atherosclerosis accounts for more than 95% of cases [19].
| Materials and Methods | ▴Top |
Eligibility criteria
The selection of studies for this systematic review and meta-analysis adhered to the stringent PICOS (Population, Intervention, Comparison, Outcome, and Study Design) framework, as recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [20]. Inclusion and exclusion criteria are mentioned in Table 1.
 Click to view | Table 1. Inclusion and Exclusion Criteria |
Inclusion criteria
1) Peer-reviewed studies published within the last 5 years, comparing the efficacy of PCI versus CABG, were included. 2) Only RCTs with accessible abstracts and full texts were considered. 3) Studies in English and Russian were selected to encompass a broad range of global research. 4) Patient populations included those with IHD, specifically cases involving triple-vessel CAD and left main coronary artery occlusion. 5) Eligibility extended to patients with a degree of stenosis above 70%, or progression from 50% to 70% stenosis within 5 years. 6) A SYNTAX score of 32 or higher was required for inclusion, signifying a complex coronary artery condition.
Exclusion criteria
1) Studies published before 2018 were excluded to focus on the most recent and relevant data. 2) Case reports, cohort studies, and other observational studies were not considered, to prioritize the highest quality of evidence. 3) RCTs reporting significant comorbidities were excluded to isolate the effects of the interventions on the specific conditions of interest. 4) Patients with a SYNTAX score below 32 were not included, ensuring a focus on more complex coronary artery cases. 5) Consistent with SYNTAX trial protocols, patients experiencing acute pre-procedural MI were excluded from consideration.
Information sources
For the comprehensive identification of relevant literature, an extensive search was conducted across multiple renowned databases. These included PubMed, Cochrane Library, and Google Scholar, among others, chosen for their wide range of scientific and medical publications. Additionally, we expanded our search to encompass various independent academic journals known for their contributions to cardiovascular research. However, it is noteworthy that despite considering these additional sources, no articles were included from these independent journals in our final selection due to the unavailability of full-text versions. This approach in selecting databases and journals ensured a broad and thorough coverage of the existing literature, thereby enriching the quality and comprehensiveness of our systematic review and meta-analysis.
Search strategy
Our search strategy was carefully formulated to encompass a wide array of studies pivotal to our research aims. This exhaustive search spanned several databases, leading to the identification of 32 studies involving a total of 1,039 participants, which closely matched our predefined search parameters. We structured our search criteria to incorporate a balanced mix of key terms and phrases, targeting areas central to our research focus.
Moreover, our search was not limited to mere database exploration. We extended our scrutiny to the reference lists of all studies included in our review. This additional step was imperative in unearthing further studies of relevance, potentially overlooked in our initial search efforts. Such thoroughness was instrumental in broadening the scope and enhancing the depth of our literature review, thereby enriching our understanding and analysis.
The precision of our search, coupled with the exhaustive nature of our approach, ensured the inclusion of the most pertinent and specific studies in our field. Through this methodical process, we have established a foundation of comprehensive and high-quality research integral to our systematic review and meta-analysis.
For an in-depth overview of our search strategy, detailing the nuanced approach and specific methodologies employed, we invite readers to consult Supplementary Material 1 (www.cardiologyres.org). This document is a testament to our thorough approach, affirming our commitment to a rigorous and comprehensive exploration of the literature.
Selection process
The selection process for relevant literature was conducted, focusing on peer-reviewed journals and publications that met our predetermined inclusion criteria. We prioritized journals with high-impact factors to minimize publication bias, ensuring the inclusion of high-quality and influential studies. The Consolidated Standards of Reporting Trials (CONSORT) for clinical trials and PRISMA for systematic reviews and meta-analyses are two examples of established publication standards and reporting criteria that are frequently followed by high-impact journals. These recommendations facilitate the identification and resolution of potential biases in study design, conduct, and analysis by promoting transparency, completeness, and accuracy in presenting research techniques and outcomes. To streamline the selection process, all identified articles were uploaded to Rayyan.ai, a specialized platform for systematic review management [21]. This facilitated efficient primary and secondary screening of the literature.
The initial phase involved the identification and removal of duplicate studies, which resulted in the exclusion of 66 articles, thereby preventing redundancy and potential bias in our analysis. Subsequently, using the platform’s automation tools, 437 articles were marked as ineligible based on predefined criteria. This left us with 422 articles that were subjected to primary screening.
A team of researchers collaboratively undertook the task of reviewing these articles. This collaborative effort ensured a comprehensive and unbiased assessment, leading to the inclusion or exclusion of studies based on a consensus that adhered strictly to our inclusion and exclusion criteria. Ultimately, 32 studies were selected for the final review and analysis.
Revascularization
The exclusion of certain studies was based on several key factors: 1) inadequacy of the study design for our analysis; 2) lack of alignment with the preferred outcomes of our study; and 3) identification of a significant risk of bias (ROB). In some cases, a combination of these factors influenced the decision to exclude a study. This rigorous selection process was pivotal in ensuring that only the most relevant, reliable, and high-quality studies were included in our systematic review and meta-analysis.
Data items
Upon completing the secondary screening of the literature, we evaluated the 32 selected articles. In line with the PRISMA guidelines, we developed a PRISMA flow diagram to systematically illustrate the study selection process. This diagram, detailed in Figure 1 [20], visually represents the inclusion and exclusion of studies from the initial pool to the final selection, ensuring transparency and clarity in our methodology.
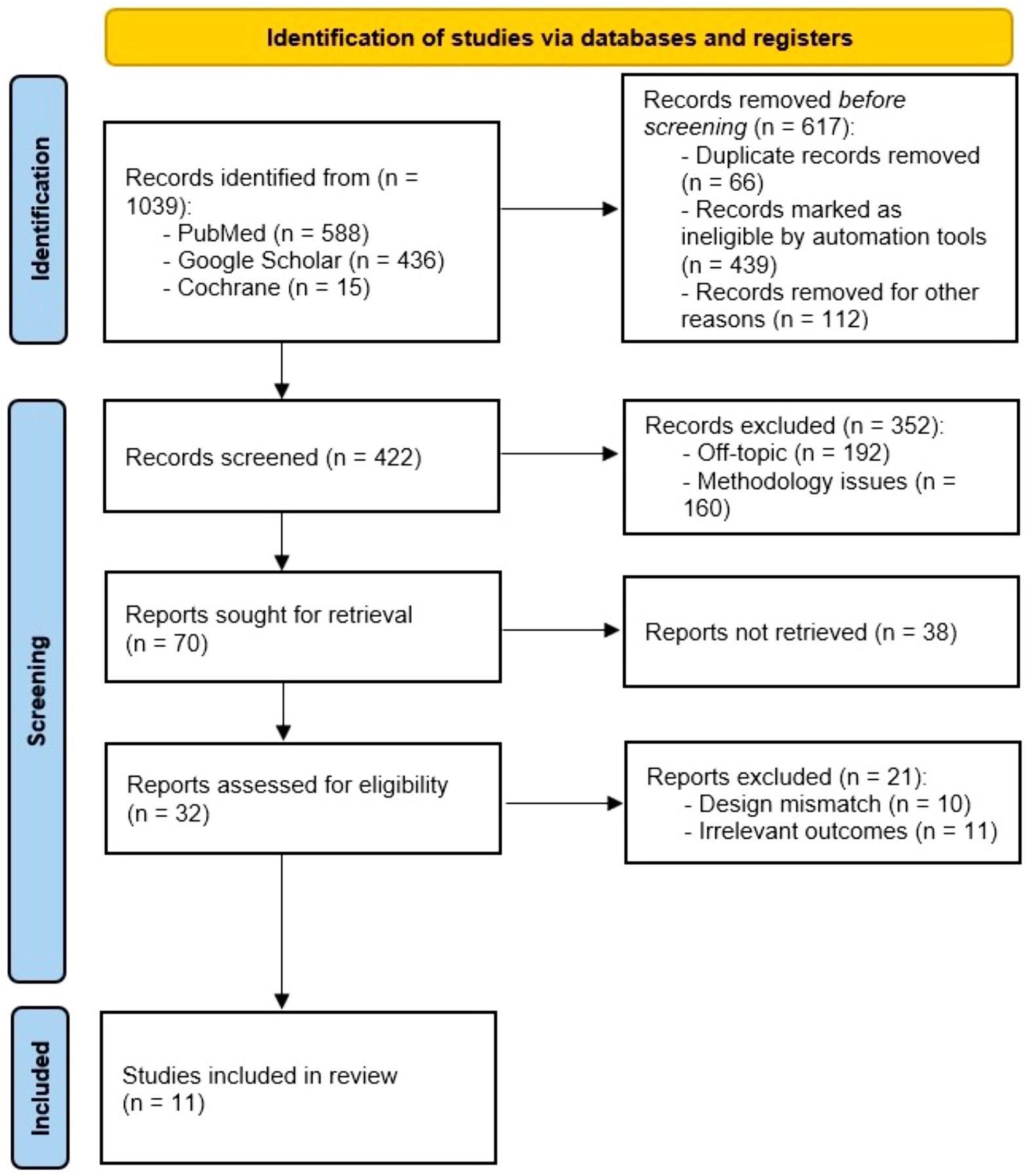 Click for large image | Figure 1. PRISMA flowchart illustrating the study selection process. |
Subsequently, we systematically tabulated the interventions from each study against their respective study populations and outcomes. This was done to ensure a detailed and organized synthesis of the data. The synthesis table specifically highlights the key themes and findings from these outcomes, providing a clear overview of the study’s results.
In our effort to minimize bias in the analysis, we employed several strategies: 1) we focused on including high-quality research, ensuring robustness in our findings; 2) all peer-reviewed studies were required to disclose any conflicts of interest, adding a layer of transparency; 3) we addressed potential biases related to informed consent and peer review processes in clinical research, thereby upholding ethical standards; 4) preference was given to meta-analyses over ordinary review articles, as they offer a more comprehensive and systematic evaluation of available data; and 5) systematic reviews and narrative reviews were generally excluded to maintain focus on primary research studies, by Dickersin, 1997 guidelines for mitigating publication bias.
To visually summarize the ROB assessment and facilitate an easy interpretation of the data, a “traffic light” figure was created. This figure serves as an intuitive tool for quickly understanding the risk levels across different studies, thus aiding collaborators and readers in evaluating the reliability of the findings. The summary of the ROB, indicating potential biases in the studies, is conveniently included for reference and review by collaborators.
Quality assessment
Systematic review
For the systematic review, publication bias was rigorously examined in all selected studies, crucial for ensuring the quality of our assessment. This involved detailed reviews of population demographics, outcome domains, and intervention characteristics for each study. The ROB was independently assessed using the Cochrane Risk of Bias criteria, a well-established method in research. We utilized the Cochrane Risk of Bias tool (2019 version) [22], following the methodology outlined by Higgins et al (2011). This process involved evaluating potential biases across five key domains: 1) biases from the randomization process; 2) deviations from intended interventions; 3) missing outcome data; 4) outcome measurement inaccuracies; and 5) selection biases in reporting results. This comprehensive approach assures a thorough and unbiased evaluation of the studies under review.
Meta-analysis
In the meta-analysis, the Cochrane Risk of Bias tool (version 3.5.1) was used to evaluate potential biases in the primary studies. This tool allowed us to assess seven critical domains of risk: 1) random sequence generation to counter selection bias; 2) allocation concealment for additional protection against selection bias; 3) blinding of participants and personnel to reduce performance bias; 4) blinding of outcome assessment for minimizing detection bias; 5) analysis of incomplete outcome data for attrition bias; 6) consideration of selective reporting to identify reporting bias; and 7) identification of any other biases. Utilizing dichotomous data extracted from 11 studies, this assessment was integral to the validity of our meta-analysis. To visually represent our findings, we employed Review Manager (RevMan version 5.4) [23], producing forest plots that offer a clear and comprehensive view of our analytical results.
Ethics
An Institutional Review Board approval and ethical compliance with human or animal studies is not required for a meta-analysis study, because it is a research methodology that uses already published and publicly available data.
| Results | ▴Top |
Data extraction
A structured data collection form was created using Microsoft Excel to systematically capture all relevant data points and outcomes from the included studies. This form was designed to include essential variables such as the clinical trial phase, publication year, sample size, baseline participant characteristics, primary outcomes, and any noted adverse events. Each selected article underwent an independent evaluation to ensure accuracy and consistency in data extraction, facilitating a comprehensive and reliable aggregation of information critical to the study’s analysis and conclusions. This rigorous data extraction process was integral to maintaining a high standard of data integrity and validity in our meta-analysis.
Study characteristics
For the final analysis, a careful manual selection resulted in 11 high-quality studies, all of which were RCTs. This selection was aimed at ensuring the reliability and relevance of our findings. The duration of follow-up in these studies varied, ranging from a minimum of 3 months to a maximum of 60 months (5 years). This range allowed us to assess both short-term and long-term outcomes of the interventions.
The primary endpoint of our analysis focused on the incidence of revascularization in treatments involving PCI and CABG. Notably, CABG was favored as the more effective intervention in 10 out of 11 studies (91%). Conversely, one study (9%) presented a negative association with CABG, indicating a less favorable outcome in certain contexts. The sample sizes in these trials varied significantly, ranging from as few as 53 participants to as many as 948, providing a broad perspective on the subject.
For the secondary endpoints of stroke and MI, the data also revealed insightful trends. PCI was favored for reducing stroke incidences in four out of five studies (80%), while CABG was preferred for reducing MI in six out of seven studies (86%). However, there were instances where one out of five studies (20%) for stroke and one out of seven studies (14%) for MI showed either no significant effect or a negative association. The sample sizes for these secondary endpoints ranged from 49 to 957 participants.
To provide a comprehensive understanding of the outcomes, we tabulated the results of these studies against their respective variables of interest, considering the entire range of sample sizes. Furthermore, the baseline characteristics and key data points from these 11 studies have been systematically compiled and are presented in Table 2 [22-32] and Table 3 [22-26, 28, 30-32]. They offer an organized overview of the study characteristics, facilitating an easier comparison and interpretation of the research findings.
Click to view | Table 2. Systematic Review Findings |
Click to view | Table 3. Patient Demographics and Clinical Characteristics |
ROB assessment
The detailed outcomes of our ROB assessment are comprehensively visualized in Figure 2 [22-32].
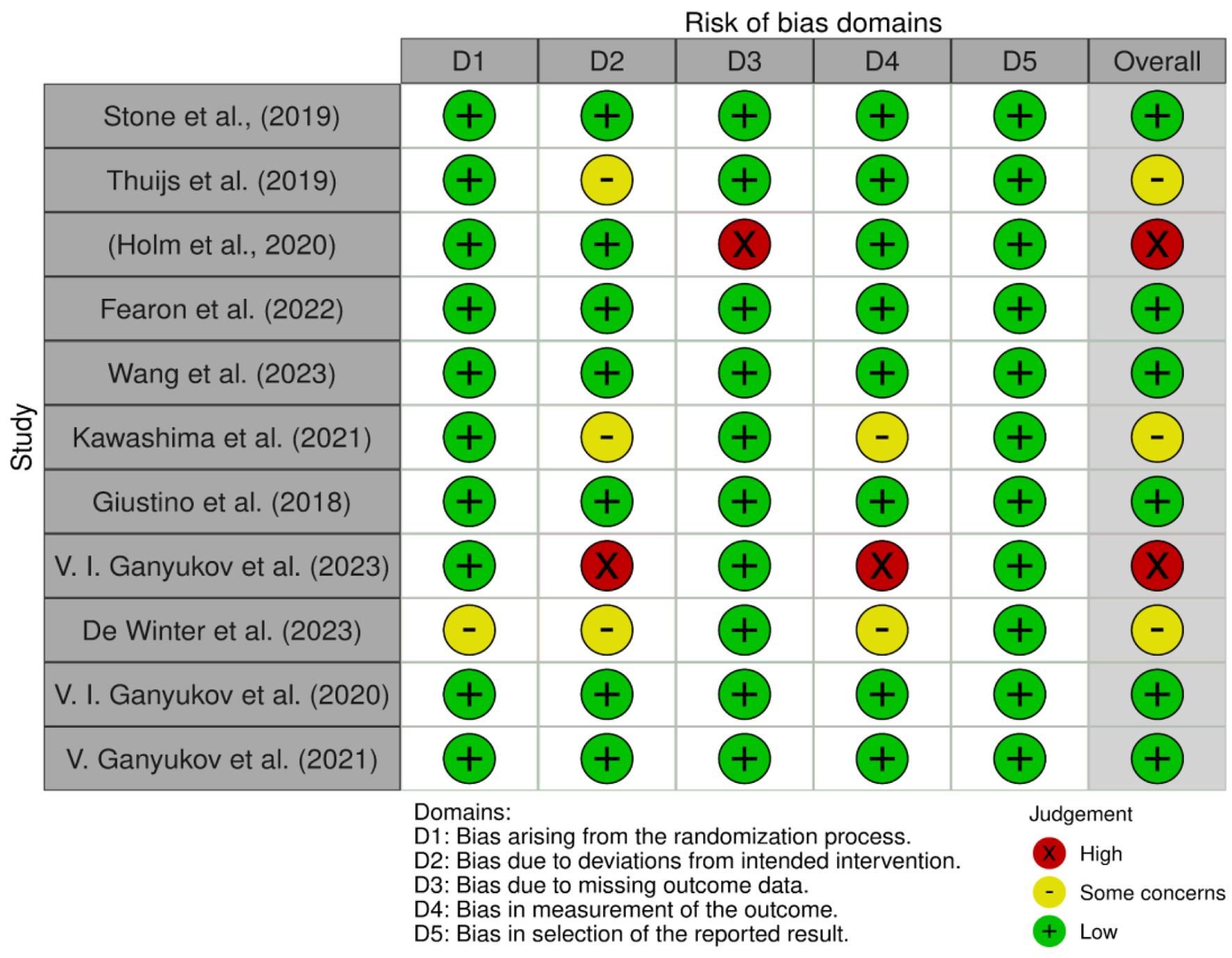 Click for large image | Figure 2. Cochrane ROB traffic light plot [22-32]. ROB: risk of bias. |
Forest plots
For our meta-analysis, forest plots were constructed using data from 11 distinct studies. These plots were designed to visually represent the primary outcomes, quantified through the Mantel-Haenszel (M-H) method under a random effects model. The confidence intervals (CIs) of 95% were calculated and depicted along the horizontal axis of each plot. The green squares on the plots symbolize the point estimations for each study, providing a clear, concise visual representation of the data. Central to each forest plot is a vertical line, which signifies the line of no effect, serving as a reference point to easily discern the direction and magnitude of the effects observed in the studies. This graphical representation is crucial for intuitively understanding and interpreting the aggregated data from multiple studies, thereby enhancing the clarity and accessibility of our research findings.
PCI vs. CABG
In our analysis, the sample sizes for the treatment groups were closely matched, with 5,734 participants receiving PCI and 5,730 undergoing CABG. The primary endpoint for this comparison was the incidence of revascularization, evaluated using KM scores. Notably, a significant majority of the studies, 10 out of 11 (91%), showed a preference for CABG over PCI, with only one study (9%) favoring PCI. The aggregated M-H value, calculated to be 1.85 with a 95% CI of 1.65 - 2.07, underscored CABG’s superiority. The data exhibited minimal heterogeneity, primarily attributed to one study with lesser weight [33]. The heterogeneity metrics were Tau2 = 0.00, Chi2 = 7.25, degrees of freedom (df) = 10, and I2 = 0%, indicating a consistent pattern across the studies. The overall effect size was significant (Z = 10.74, P = 0.001), suggesting that CABG is more effective in reducing revascularization rates compared to PCI.
The individual M-H values from studies such as Stone et al (2019), Thuijs et al (2019), Ganyukov et al (2020), Giustino et al (2020), and Holm et al (2020) ranged between 1.83 (CI: 1.39 - 2.41) and 1.84 (CI: 1.30 - 2.59), reinforcing the trend. Other studies, including Kawashima et al (2021), Fearon et al (2022), and Wang et al (2023) presented M-H values from 1.56 (CI: 0.96 - 2.51) to 2.30 (CI: 1.79 - 2.96), further corroborating the effectiveness of CABG in this context.
This comprehensive analysis establishes a clear positive association between CABG and improved revascularization outcomes, suggesting that PCI, in comparison, may lead to less favorable clinical results when revascularization is the primary endpoint of concern (Figs. 3 and 4) [22-32].
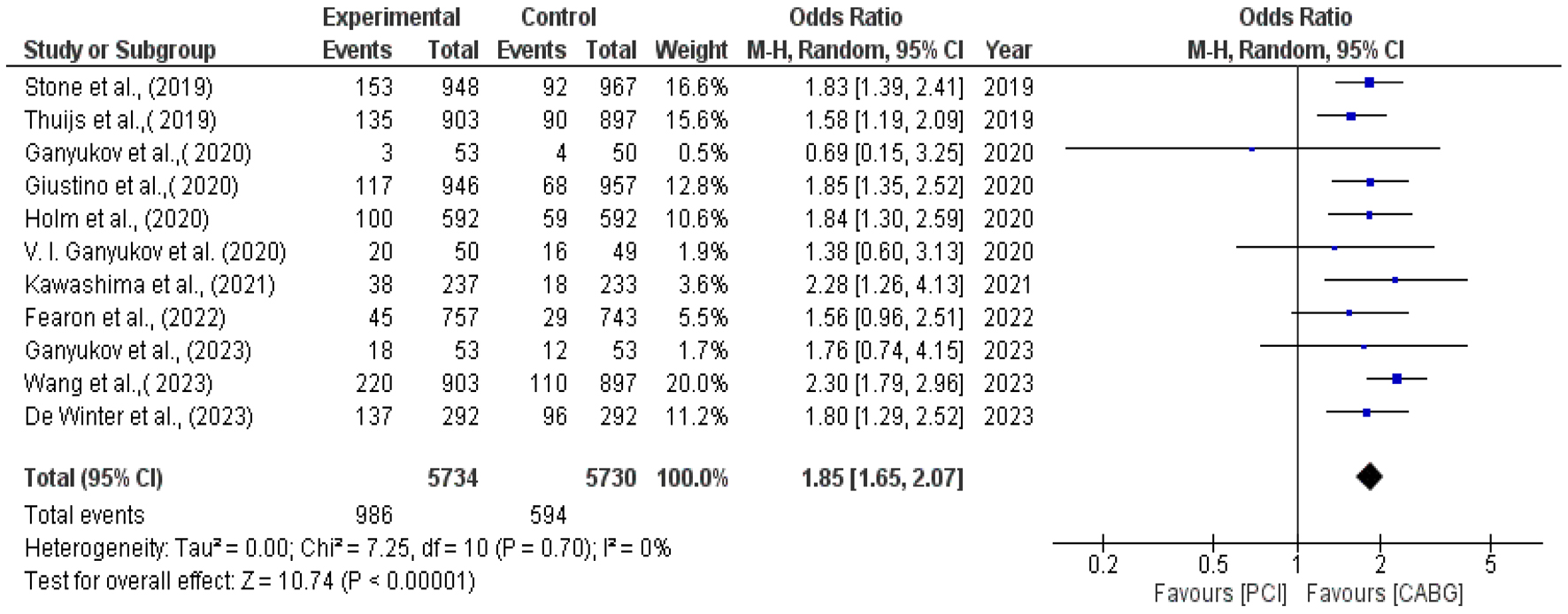 Click for large image | Figure 3. Forest plot for primary endpoint: repeat revascularization [22-32]. |
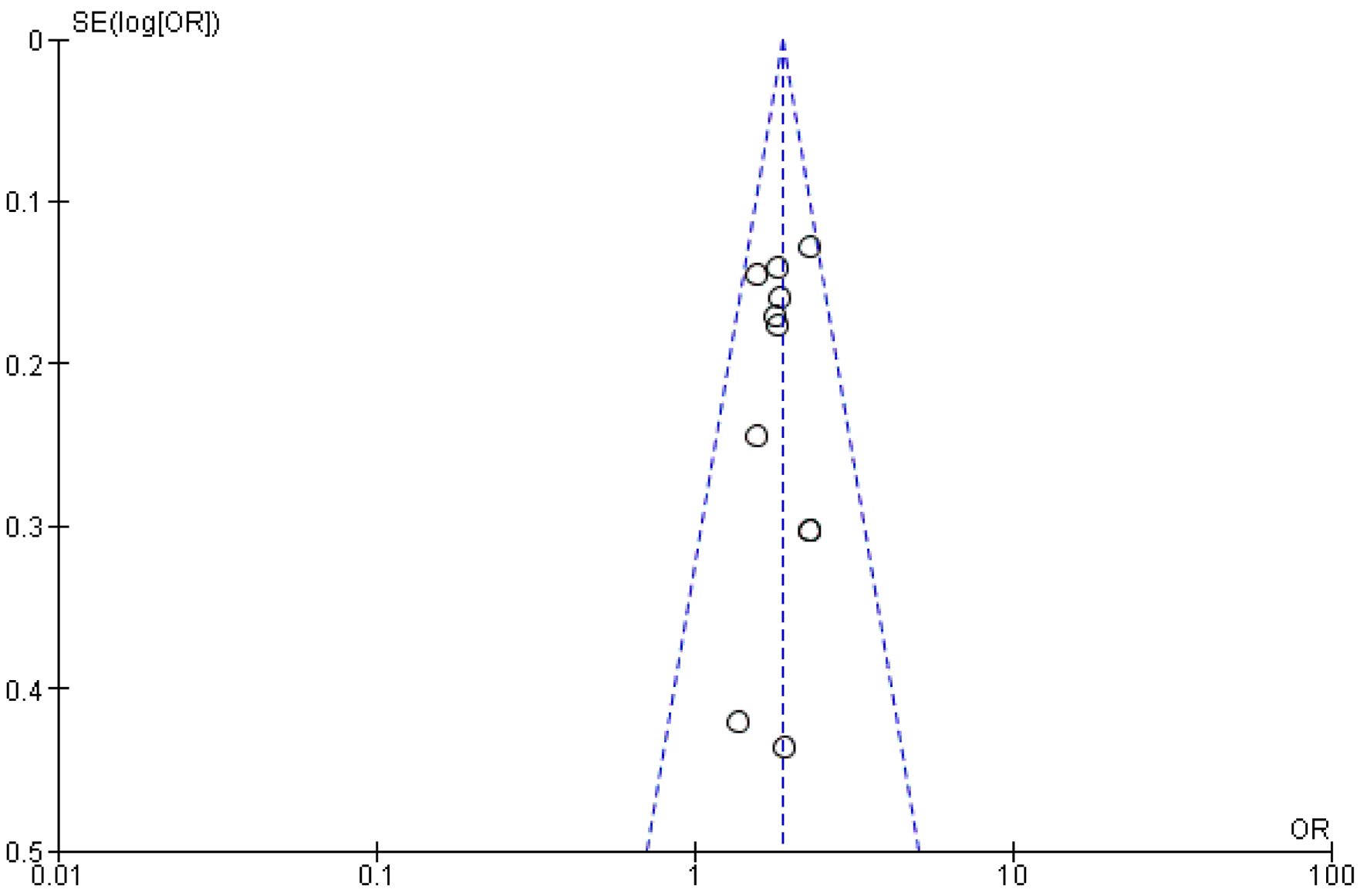 Click for large image | Figure 4. Funnel plot analysis for revascularization. |
Stroke
In evaluating the impact of PCI and CABG on stroke outcomes, our study involved closely matched sample sizes, with 2,711 patients in the PCI group and 2,699 in the CABG group. The analysis revealed a clear trend favoring PCI for stroke reduction, with four out of five studies (80%) supporting PCI, while only one out of five (20%) indicated a preference for CABG. The pooled M-H value for stroke was calculated to be 0.80, with a 95% CI of 0.60 - 1.10, suggesting a lower risk of stroke with PCI.
The heterogeneity across these studies was minimal, primarily influenced by one study with lesser weight [33]. The overall heterogeneity metrics indicated a consistent pattern, with Tau2 = 0.00, Chi2 = 1.19, df = 4, and I2 = 0%. The calculated effect size was Z = 1.33 (P = 0.18), which, while significant, had a limited P-value, indicating a need for cautious interpretation. The individual M-H values from studies such as Fearon et al (2022), Stone et al (2019), and Thuijs et al (2019) ranged between 0.70 (CI: 0.27 - 1.83) and 0.86 (CI: 0.31 - 2.38), further supporting the advantage of PCI in reducing stroke risk.
This analysis conclusively shows a positive association between PCI and a reduced risk of stroke, suggesting that CABG may lead to comparatively less favorable outcomes in terms of stroke risk when evaluated as a secondary endpoint (Figs. 5 and 6) [22, 23, 25, 29, 32].
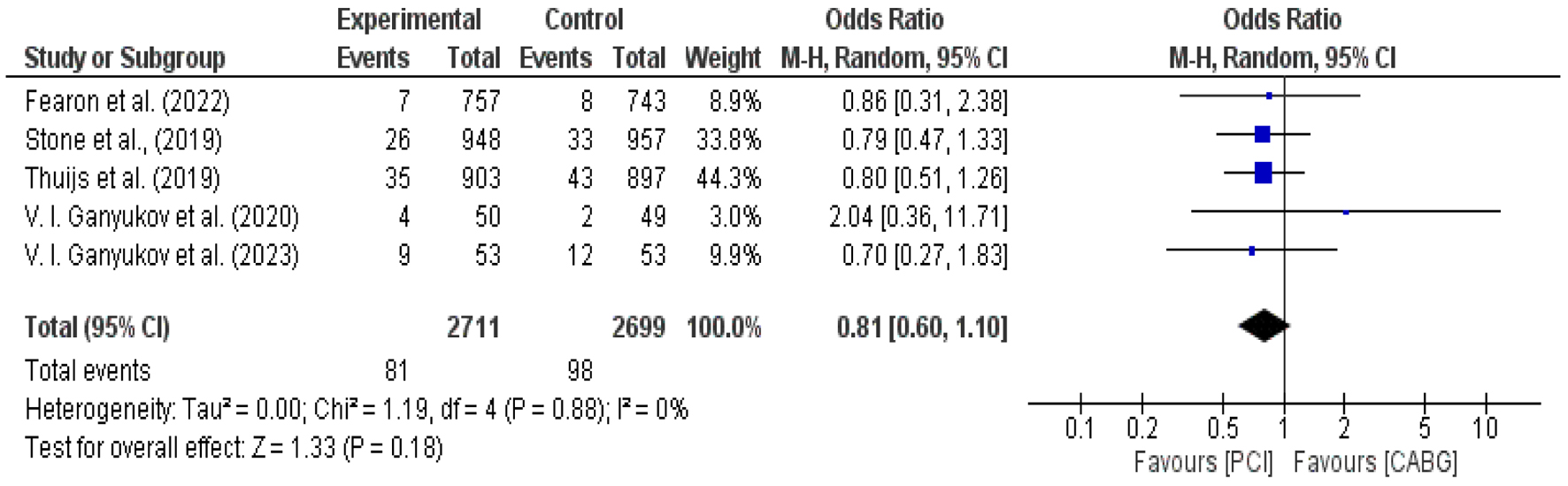 Click for large image | Figure 5. Forest plot for incidence of stroke in PCI vs. CABG [22, 23, 25, 29, 32]. CABG: coronary artery bypass grafting; PCI: percutaneous coronary intervention. |
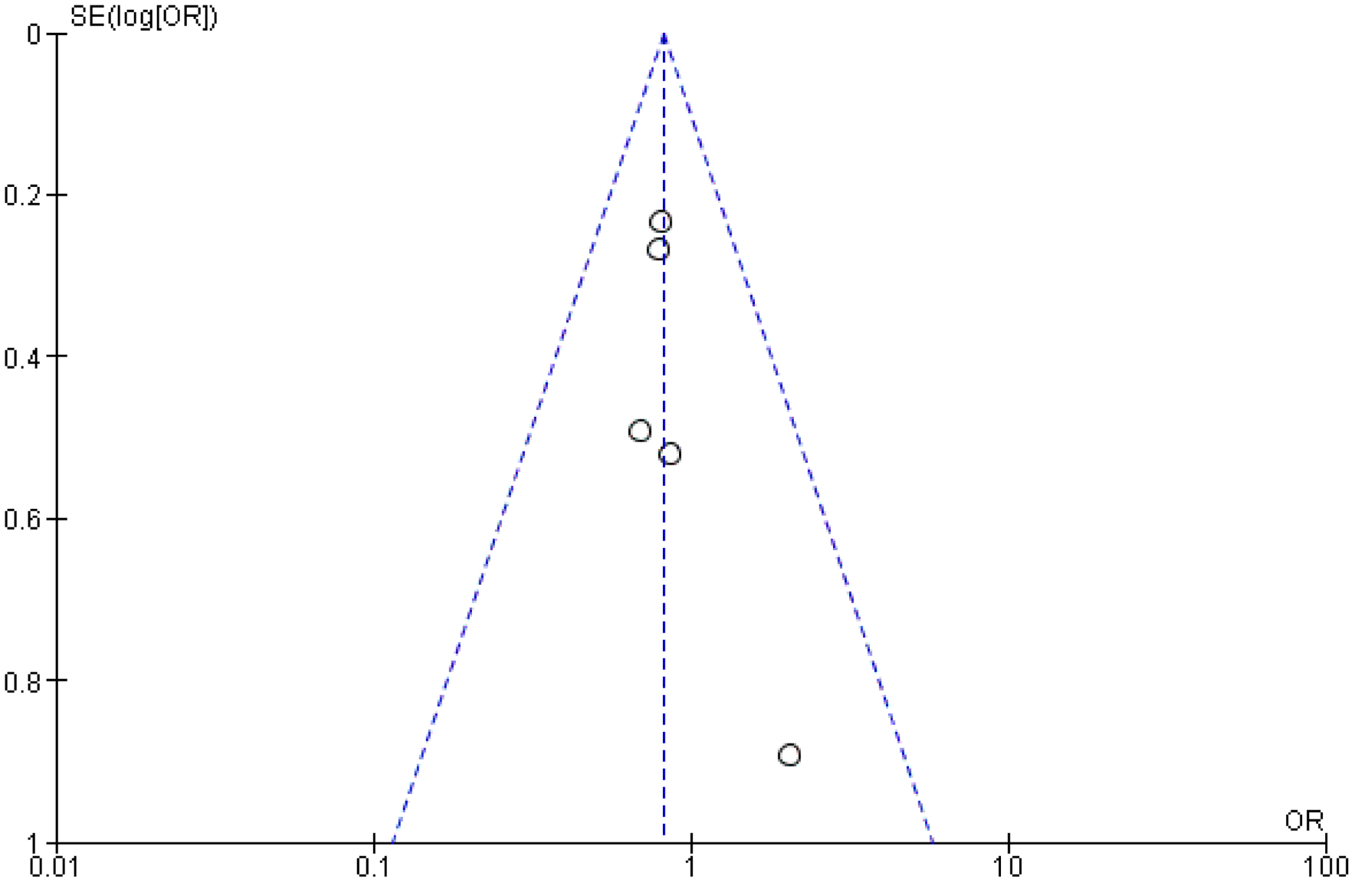 Click for large image | Figure 6. Funnel plot analysis for stroke. |
MI
In assessing the impact of CABG and PCI on MI outcomes, our study analyzed data from a comparable number of patients in each group, with 3,356 in the PCI cohort and 3,341 in the CABG cohort. The findings significantly favored CABG, with six out of seven studies (86%) advocating for its efficacy in reducing post-procedural MI, as opposed to just one out of seven studies (14%) supporting PCI.
The aggregated M-H value for MI was 2.71, with a 95% CI of 1.13 - 6.53, suggesting a substantial reduction in the incidence of MI with CABG compared to PCI. The data presented notable heterogeneity, contributed by multiple studies including several iterations by Ganyukov et al [29, 31, 32, 34]. The heterogeneity metrics showed Tau2 = 1.18, Chi2 = 86.88, df = 6, and a high I2 value of 93%, indicating considerable variability across the studies. Despite this, the overall effect size was Z = 2.47 (P < 0.05), which is statistically significant, underscoring a trend favoring CABG.
The individual M-H values from studies such as Holm et al (2020), Fearon et al (2022), and Stone et al (2019) further validate this trend, with values ranging from 0.94 (CI: 0.22 - 3.97) to 9.16 (CI: 6.54 - 12.83), reinforcing the conclusion that CABG is associated with a lower incidence of post-procedural MI compared to PCI. This analysis establishes a clear positive correlation between CABG and reduced MI rates, indicating that CABG may be the more effective option for minimizing the risk of MI as a secondary endpoint in IHD treatment (Figs. 7 and 8) [22-25, 29, 31, 32].
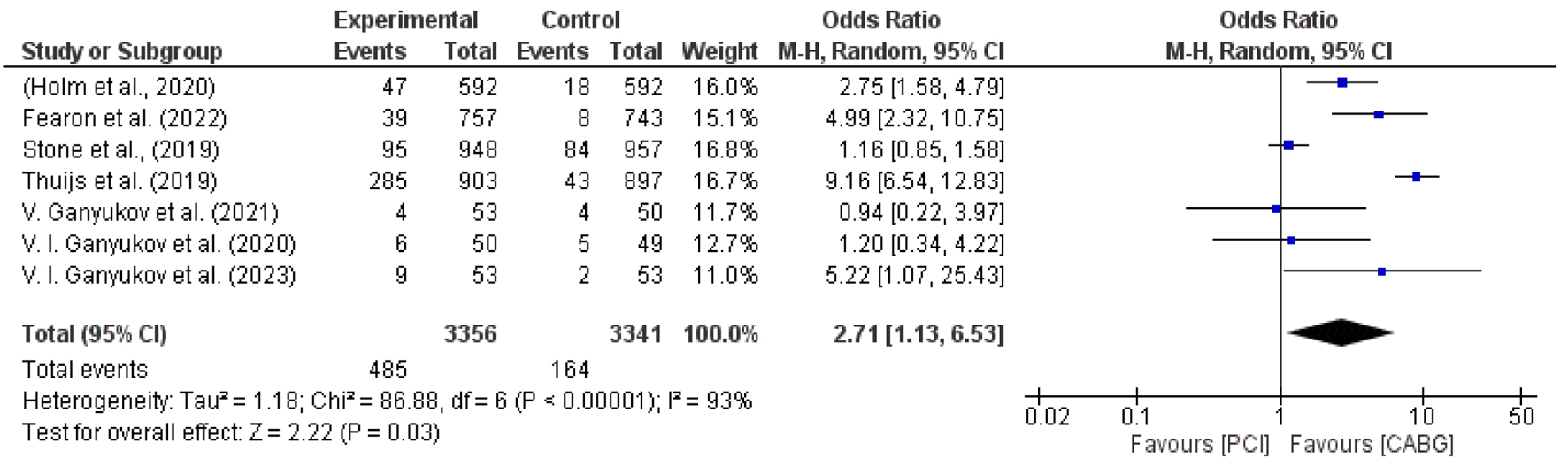 Click for large image | Figure 7. Forest plot for incidence of myocardial infarction among PCI vs. CABG [22-25, 29, 31, 32]. |
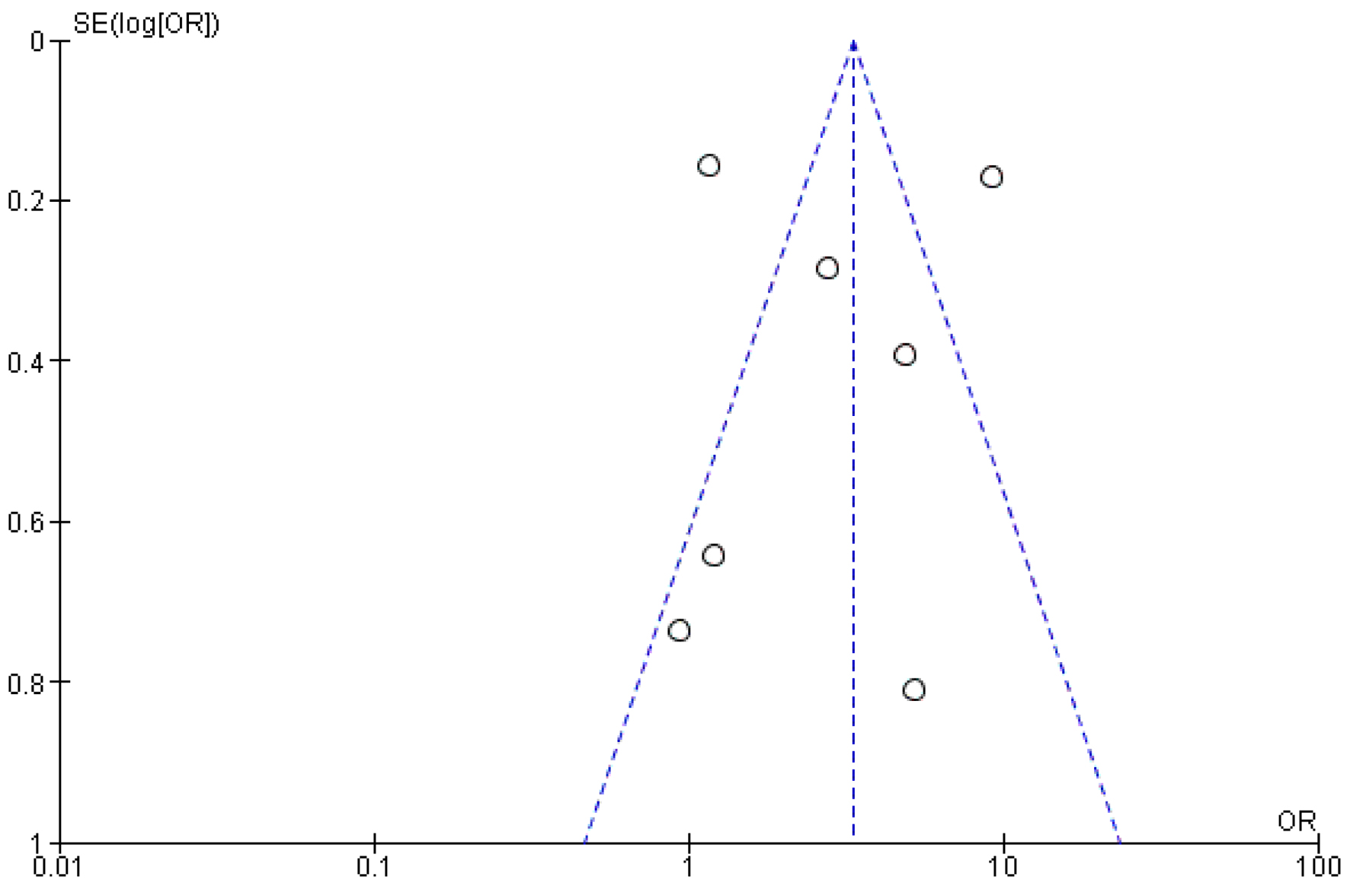 Click for large image | Figure 8. Funnel plot analysis for myocardial infarction. |
| Discussion | ▴Top |
The current systematic review and meta-analyses aimed at providing a comprehensive evaluation in identifying the more efficacious mode of intervention among PCI and CABG in the context of IHD. The “efficacy” is determined by the relative decrease in the incidence of revascularization, which was set as the primary endpoint in our study, and the decrease in the incidence of post-procedural stroke/SE and MI, the secondary endpoints of our study. Various studies on PCI and CABG were more focused on determining the major adverse cardiac and cerebrovascular events (MACCEs) among both treatment groups. We extracted the desirable outcomes from these studies for revascularization, stroke, and MI.
In the study conducted by Stone et al (2019), a total of 1,905 patients with left main CAD were randomly assigned to PCI and CABG with 948 and 957 patients in both trials, respectively. To characterize the long-term outcomes of revascularization of both PCI and CABG, the point estimation for data extraction was set at a 5-year follow-up. Ischemia-driven revascularization was more frequent after PCI than after CABG (16.9% vs. 10.0%; difference, 6.9 percentage points; 95% CI: 3.7 - 10.0), hence, showing a more favorable outcome with CABG than PCI. The overall effect size was found to be Z = 10.74 (P = 0.001), which was significant. In another study by Thuijs et al (2019), which was conducted across 18 North American and European Hospitals, the SYNTAX score was used to characterize patients with coronary artery complexity, with scores of 22 or less defined as low, 22 - 32 as intermediate, and higher than 32 as greater. The effect size of this study was found to be Z = 1.58 (95% CI: 1.19 - 2.09) in favor of CABG.
Another study by Giustino et al (2020) with a 3-year follow-up period showed that PCI was associated with higher rates of any repeat revascularization (12.9% vs. 7.6%; hazard ratio (HR): 1.73; 95% CI: 1.28 - 2.33; P = 0.0003). According to the study by Holm et al (2020), repeat revascularization was estimated at 17% after PCI versus 10% after CABG (HR 1.73 (95% CI: 1.25 - 2.40); P = 0.0009), also demonstrating the relative decrease in the incidence of revascularization with CABG. A study by Ganyukov et al (2020) also showed similar outcomes. Kawashima et al (2021) had a sample size of 2.28 (95% CI: 1.26 - 4.13) and Fearon et al (2022) had 1.56 (95% CI: 1.26 - 4.13) respectively. Repeat revascularization was estimated in 17% after PCI versus 10% after CABG (HR 1.73 (95% CI: 1.25 - 2.40); P = 0.0009). In contrast to this, the study by Ganyukov et al (2020) indicated that PCI had a better prognosis than CABG because, at the end of 3 years, the occurrence of the primary endpoint was 98% and 94.3%, for CABG and PCI respectively among the included patients. This study had an effect size of Z = 0.69 (95% CI: 0.15 - 3.250). The study by Ganyukov et al (2023), Wang et al (2023), and De Winter et al (2023) also favored CABG, indicating overall that CABG is more efficacious than PCI. In a study [35] which was a meta-analysis conducted in 2021, the revascularization rate was also compared among the treatment groups, but the studies used were all observational studies. Our meta-analyses used only RCTs, which eliminates the risk of confounding bias, making it highly unlikely.
This preference results from several important variables that demonstrate how much better CABG is than PCI at producing more comprehensive and long-lasting revascularization. First off, diseased coronary segments can be bypassed with venous or arterial grafts thanks to CABG, which opens up new blood vessels that supply the myocardium. When opposed to PCI, which may have limitations due to the quantity and size of target arteries that can be stented, this method offers a more thorough treatment of multi-vessel illness. Research has demonstrated that CABG reduces the need for repeat procedures by achieving a higher incidence of full revascularization, which addresses all major coronary lesions. Furthermore, CABG is less likely to experience in-stent restenosis, a typical PCI complication that frequently calls for additional procedures. The incidence of restenosis after PCI has decreased with the introduction of drug-eluting stents; however, issues with late stent thrombosis and the requirement for prolonged dual antiplatelet medication still need to be addressed since they may raise the risk of bleeding and other unfavorable outcomes. The results of CABG have also been further enhanced by recent developments in perioperative care, graft selection, and surgical procedures, which makes it a desirable alternative for patients with CAD who wish to minimize the need for repeat revascularization. Although little research has been done, people who have had CABG in the past have a low rate of STEMI. Based on prior evidence, patients with post-CABG acute coronary syndrome (ACS) were more likely to present with NSTEMI (61.9%) or unstable angina (32.7%) than with STEMI (5.4%) [33].
In the comparative analysis of the efficacy of both treatment groups based on the secondary endpoint, stroke was interestingly different compared to the incidence of repeat revascularization. Patients are constantly monitored for stroke symptoms and signs in the initial postoperative period after the surgery. This includes checking vital signs, evaluating focal neurological abnormalities, and performing a neurological assessment. To confirm the diagnosis, any suspected cases of stroke are quickly evaluated using imaging tests like computed tomography (CT) or magnetic resonance imaging (MRI). In the previous meta-analyses [35], there was no difference observed in the risk of stroke. However, in our meta-analysis, 4/5 (80%) studies showed a favorable prognosis with PCI as compared to CABG. A study by Thuijs et al (2019) having an effect size of 0.80 (95% CI: 0.51 - 1.26) showed less frequent incidence of stroke among PCI. Previous meta-analyses [36] reported there was no significant incidence of stroke in PCI compared to CABG using outdated meta-analyses. For this outcome, we used clinical outcomes which were updated until the last 5 years, to report the patient prognosis with PCI, including Stone et al (2019), Fearon et al (2022), and Ganyukov et al (2023). Only 1/5 studies showed different outcomes, favoring CABG over PCI and carrying the least weight of all. When compared to the higher incidence linked to CABG, the observed drop in stroke incidence after PCI highlights a crucial component of the relative efficacy and safety profiles of both revascularization techniques. There is always a chance of embolization during CABG, especially when the damaged coronary arteries and aorta are being operated on. Furthermore, cerebral hypoperfusion and microembolization can result from aortic manipulation and cardiopulmonary bypass, which puts patients at risk for perioperative stroke. The observed difference in stroke incidence between CABG and PCI highlights the need to treat patients with CAD according to their specific requirements.
In the previous meta-analyses, no statistical difference was observed between the RCTs and observational studies used in the respective analyses [35]. Our meta-analyses used only RCTs and showed a statistically significant higher rate of MI with PCI, indicating a more favorable prognosis with CABG. In the study of Holm et al (2020), MI was estimated at 8% after PCI versus 3% after CABG (HR 2.99 (95% CI: 1.66 - 5.39); P = 0.0002). A study by Fearon et al (2022) presented a more significant reduction in MI, with a sample size of Z = 4.99 (95% CI: 2.32 - 10.75). Other studies, Stone et al (2019) and Thuijs et al (2019), also showed similar outcomes. Two other studies conducted by the same author, Ganyukov et al (2020) and Ganyukov et al (2023), with similar efficacy, were analyzed as well. Only one study, Ganyukov et al (2021), showed a negative association with CABG, but this effect size was overpowered by the other studies mentioned. In CABG, damaged parts of the coronary arteries are efficiently bypassed by creating bypass grafts that reroute blood flow around clogged coronary arteries using venous or arterial conduits. Offering more robust and permanent revascularization than PCI lowers the risk of recurrent MI by restoring blood flow to ischemic cardiac tissue. PCI can effectively relieve acute ischemia and restore blood flow to the damaged myocardium, but its effectiveness may be restricted over time by untreated coronary artery lesions developing residual stenosis, or stent restenosis. When patients have multiple vessels involved or severe CAD, these characteristics may increase the likelihood of recurrent MI after PCI as opposed to CABG.
The current study elaborated that 1) the revascularization rate is improved with CABG as compared to PCI; 2) there is a decreased incidence of stroke with PCI, and it also showed non-inferiority (P = 0.18); and 3) the post-procedural MI rate was less frequent in CABG. The current study reaffirms the superiority of CABG over PCI.
Strengths
The meta-analysis was underpinned by the use of up-to-date RCTs, which significantly mitigates the risk of confounding factors influencing the outcomes. The rigorous application of inclusion and exclusion criteria further enhanced the quality and reliability of the research, effectively minimizing potential biases. The exclusive use of RCTs also ensured higher ethical standards, as participants were randomly allocated to treatment groups, thereby reducing the likelihood of treatment bias. Additionally, the strength of this study is reflected in its internal validity, achieved through the selection of RCTs with smaller sample sizes, which typically experience lower attrition rates compared to larger observational studies. This careful selection process contributes to the robustness and credibility of the study’s findings.
Limitations
This study aligns with previous research but encounters several notable limitations that warrant consideration. The relatively small sample size restricts the generalizability of our findings to a broader population, which is crucial as larger sample sizes often provide more robust and widely applicable results. Moreover, our review did not differentiate between levels of vascular wall involvement or conduct subgroup analyses based on demographic characteristics such as age, gender, and ethnicity. Numerous studies have demonstrated that these demographic factors can substantially influence outcomes, suggesting that our results might not comprehensively represent the diverse patient population affected by IHD.
Additionally, the existing literature did not provide sufficient data to allow for the creation of sub-groups based on markers for PCI or CABG such as the type of coronary lesion or ejection fraction. This lack of specific data prevented a nuanced analysis of which subsets of patients might benefit more from one procedure over the other, thereby limiting the depth of our conclusions.
The study also did not account for the presence of comorbidities or other risk factors that often coexist with IHD. These factors can have a profound impact on treatment efficacy and patient outcomes. The exclusion of such variables in our analysis may oversimplify the complex clinical picture of IHD patients, potentially leading to an incomplete understanding of the real-world effectiveness of PCI and CABG.
The studies included in this review did not provide differentiation between the types or severities of MI and stroke events. This lack of detailed categorization prevents a nuanced understanding of how different clinical presentations of MI and stroke might respond to the interventions studied. Additionally, the studies did not specify whether diagnoses were confirmed by specialists such as neurologists, which could influence the reliability of the diagnostic data reported.
In conclusion, while this study offers valuable insights into the comparative efficacy of PCI and CABG, the findings should be interpreted with caution, considering these limitations. Future research with larger and more diverse populations, including a comprehensive analysis of comorbidities and demographic factors, is essential for a more nuanced understanding of the best treatment modalities for IHD.
Conclusion
The results of our study demonstrate the enhanced efficacy of CABG over PCI in treating IHD. CABG’s superiority is particularly evident in its ability to reduce the frequency of repeat revascularization and MI, while PCI is more advantageous in lowering the risk of stroke. CABG provides a more lasting and comprehensive solution for revascularization, significantly diminishing the likelihood of future ischemic episodes, making it a preferable option for patients with extensive coronary disease. This study underscores the importance of personalized treatment strategies based on the individual needs of patients, taking into account the robust statistical findings. It also highlights the urgent need for further research to develop detailed, evidence-based guidelines that will aid in determining the most effective treatment modalities for IHD, ensuring patient-specific, optimal care.
| Supplementary Material | ▴Top |
Suppl 1. Comprehensive search strategy.
Acknowledgments
The authors have no acknowledgements to declare, reflecting the independent completion of the work.
Financial Disclosure
No funding was received for the conduct of this study or the preparation of this article, indicating that there are no financial sources to declare.
Conflict of Interest
The authors declare no conflict of interest to ensure the impartiality of the review.
Informed Consent
Not applicable.
Author Contributions
Jordan Llerena-Velastegui, MD: supervision, conceptualization, writing - original draft, writing - review and editing. Kristina Zumbana-Podaneva, MD: supervision, writing - review and editing. Sebastian Velastegui-Zurita, MD: data curation, writing - review and editing. Melany Mejia-Mora, MD: formal analysis, writing - review and editing. Juan Perez-Tomassetti, MD: formal analysis, writing - original draft, supervision. Allison Cabrera-Cruz, MD: data curation, formal analysis, writing - original draft. Pablo Haro-Arteaga, MD: data curation, formal analysis, writing - original draft. Ana Clara Fonseca Souza de Jesus, MD: data curation, writing - review and editing, methodology. Pedro Moraes Coelho, MD: data curation, writing - original draft. Cristian Sanahuja-Montiel, MD: supervision, writing - review and editing.
Data Availability
All data generated or analyzed during this study are included in this published article, and further inquiries should be directed to the corresponding author.
Abbreviations
CABG: coronary artery bypass grafting; HR: hazard ratio; IHD: ischemic heart disease; MACCEs: major adverse cardiac and cerebrovascular events; MI: myocardial infarction; PCI: percutaneous coronary intervention; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT: randomized controlled trial; ROB: risk of bias; SYNTAX: Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery (Cardiovascular Medicine)
| References | ▴Top |
- Khan MA, Hashim MJ, Mustafa H, Baniyas MY, Al Suwaidi S, AlKatheeri R, Alblooshi FMK, et al. Global epidemiology of ischemic heart disease: results from the global burden of disease study. Cureus. 2020;12(7):e9349.
doi pubmed pmc - Finegold JA, Asaria P, Francis DP. Mortality from ischaemic heart disease by country, region, and age: statistics from World Health Organisation and United Nations. Int J Cardiol. 2013;168(2):934-945.
doi pubmed pmc - Lemaire A, Soto C, Salgueiro L, Ikegami H, Russo MJ, Lee LY. The impact of age on outcomes of coronary artery bypass grafting. J Cardiothorac Surg. 2020;15(1):158.
doi pubmed pmc - Kasprzyk M, Wudarczyk B, Czyz R, et al. Ischemic heart disease - definition, epidemiology, pathogenesis, risk factors, and treatment. Postepy Nauk Medycznych [Internet]. 2018;31(06):358-360.
doi - Liga R, Colli A, Taggart DP, Boden WE, De Caterina R. Myocardial revascularization in patients with ischemic cardiomyopathy: for whom and how. J Am Heart Assoc. 2023;12(6):e026943.
doi pubmed pmc - Bangalore S, Maron DJ, Stone GW, Hochman JS. Routine revascularization versus initial medical therapy for stable ischemic heart disease: a systematic review and meta-analysis of randomized trials. Circulation. 2020;142(9):841-857.
doi pubmed - Akbari T, Al-Lamee R. Percutaneous coronary intervention in multi-vessel disease. Cardiovasc Revasc Med. 2022;44:80-91.
doi pubmed - Diodato M, Chedrawy EG. Coronary artery bypass graft surgery: the past, present, and future of myocardial revascularisation. Surg Res Pract. 2014;2014:726158.
doi pubmed pmc - Persson J, Yan J, Angeras O, Venetsanos D, Jeppsson A, Sjogren I, Linder R, et al. PCI or CABG for left main coronary artery disease: the SWEDEHEART registry. Eur Heart J. 2023;44(30):2833-2842.
doi pubmed pmc - Safarian H, Alidoosti M, Shafiee A, Salarifar M, Poorhosseini H, Nematipour E. The SYNTAX score can predict major adverse cardiac events following percutaneous coronary intervention. Heart Views. 2014;15(4):99-105.
doi pubmed pmc - Zaidat OO, Lazzaro MA, Liebeskind DS, Janjua N, Wechsler L, Nogueira RG, Edgell RC, et al. Revascularization grading in endovascular acute ischemic stroke therapy. Neurology. 2012;79(Suppl 1):13 S110-116.
doi pubmed pmc - Goel MK, Khanna P, Kishore J. Understanding survival analysis: Kaplan-Meier estimate. Int J Ayurveda Res. 2010;1(4):274-278.
doi pubmed pmc - Lu L, Liu M, Sun R, Zheng Y, Zhang P. Myocardial infarction: symptoms and treatments. Cell Biochem Biophys. 2015;72(3):865-867.
doi pubmed - Murphy SJ, Werring DJ. Stroke: causes and clinical features. Medicine (Abingdon). 2020;48(9):561-566.
doi pubmed pmc - Enrique B, Marta B. Efficacy, effectiveness and efficiency in the health care: the need for an agreement to clarify its meaning. International Archives of Public Health and Community Medicine [Internet]. 2020;4(1):035.
doi - Khan SQ, Ludman P. Percutaneous coronary intervention. Medicine [Internet]. 2022;50(7):437-444.
doi - Fleissner F, Warnecke G, Cebotari S, Rustum S, Haverich A, Ismail I. Coronary artery bypass grafting in young patients—insights into a distinct entity. J Cardiothorac Surg. 2015;10:65.
doi pubmed pmc - Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
doi pubmed pmc - Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
doi pubmed pmc - Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
doi pubmed pmc - Review Manager (RevMan) [Computer program]. Version 5.4. The Cochrane Collaboration, 2020 https://training.cochrane.org/system/files/uploads/protected_file/RevMan5.4_user_guide.pdf.
- Stone GW, Kappetein AP, Sabik JF, Pocock SJ, Morice MC, Puskas J, Kandzari DE, et al. Five-year outcomes after PCI or CABG for left main coronary disease. N Engl J Med. 2019;381(19):1820-1830.
doi pubmed - Thuijs D, Kappetein AP, Serruys PW, Mohr FW, Morice MC, Mack MJ, Holmes DR, Jr., et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet. 2019;394(10206):1325-1334.
doi pubmed - Holm NR, Makikallio T, Lindsay MM, Spence MS, Erglis A, Menown IBA, Trovik T, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020;395(10219):191-199.
doi pubmed - Fearon WF, Zimmermann FM, De Bruyne B, Piroth Z, van Straten AHM, Szekely L, Davidavicius G, et al. Fractional flow reserve-guided PCI as compared with coronary bypass surgery. N Engl J Med. 2022;386(2):128-137.
doi pubmed - Wang R, Lunardi M, Hara H, Gao C, Ono M, Davierwala PM, Holmes DR, et al. Impact of repeat revascularization within 5 years on 10-year mortality after percutaneous or surgical revascularization. Clin Res Cardiol. 2023;112(9):1302-1311.
doi pubmed pmc - Kawashima H, Takahashi K, Ono M, Hara H, Wang R, Gao C, Sharif F, et al. Mortality 10 years after percutaneous or surgical revascularization in patients with total coronary artery occlusions. J Am Coll Cardiol. 2021;77(5):529-540.
doi pubmed - Giustino G, Serruys PW, Sabik JF, 3rd, Mehran R, Maehara A, Puskas JD, Simonton CA, et al. Mortality after repeat revascularization following PCI or CABG for left main disease: the EXCEL trial. JACC Cardiovasc Interv. 2020;13(3):375-387.
doi pubmed - Ganyukov VI, Kochergin NA, Shilov AA, Tarasov RS, Kozyrin KA, Prokudina ES, Barbarash OL, et al. Randomized clinical trial of hybrid vs. surgical vs. percutaneous multivessel coronary revascularization: 5-year follow-up of HREVS trial. Kardiologiia. 2023;63(11):57-63.
doi pubmed - de Winter RW, Walsh SJ, Hanratty CG, Spratt JC, Sprengers RW, Twisk JWR, Vegting I, et al. Percutaneous coronary intervention of native coronary artery versus saphenous vein graft in patients with prior coronary artery bypass graft surgery: Rationale and design of the multicenter, randomized PROCTOR trial. Am Heart J. 2023;257:20-29.
doi pubmed - Ganyukov VI, Kochergin NA, Shilov AA, Tarasov RS, Skupien J, Kozyrin KA, Barbarash OL, et al. Randomized clinical trial of surgical versus percutaneous versus hybrid multivessel coronary revascularization: 3 years' follow-up. JACC Cardiovasc Interv. 2021;14(10):1163-1165.
doi pubmed - Ganyukov V, Kochergin N, Shilov A, Tarasov R, Skupien J, Szot W, Kokov A, et al. Randomized clinical trial of surgical vs. percutaneous vs. hybrid revascularization in multivessel coronary artery disease: residual myocardial ischemia and clinical outcomes at one year-hybrid coronary revascularization versus stenting or surgery (HREVS). J Interv Cardiol. 2020;2020:5458064.
doi pubmed pmc - Barssoum K, Kumar A, Rai D, Kharsa A, Chowdhury M, Thakkar S, Patel HP, et al. Meta-analysis comparing percutaneous coronary intervention with coronary artery bypass grafting for non-ST elevation acute coronary syndrome in patients with multivessel or left main disease. Curr Probl Cardiol. 2022;47(10):101306.
doi pubmed - Khairutdinov I, Le P, Rao N, et al. Incidence of stemi among patients with prior CABG. J Am Coll Cardiol. 2024;83(13_Supplement):1062.
doi - Shaik TA, Chaudhari SS, Haider T, Rukia R, Al Barznji S, Kataria H, Nepal L, et al. Comparative effectiveness of coronary artery bypass graft surgery and percutaneous coronary intervention for patients with coronary artery disease: a meta-analysis of randomized clinical trials. Cureus. 2022;14(9):e29505.
doi pubmed pmc - Feng S, Li M, Fei J, Dong A, Zhang W, Fu Y, Zhao Y. Ten-year outcomes after percutaneous coronary intervention versus coronary artery bypass grafting for multivessel or left main coronary artery disease: a systematic review and meta-analysis. J Cardiothorac Surg. 2023;18(1):54.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.