

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 15, Number 3, June 2024, pages 205-209

A Novel Case of Anomalous Origin of Left Vertebral Artery Associated With Left Subclavian Steal Syndrome
Poornima Vinoda, c, Hiten Patelb
aDepartment of Internal Medicine, University of North Carolina Health at Southeastern, Lumberton, NC 28358, USA
bDivision of Interventional Cardiology, University of North Carolina Health at Southeastern, Lumberton, NC 28358, USA
cCorresponding Author: Poornima Vinod, Department of Internal Medicine, University of North Carolina Health at Southeastern, Lumberton, NC 28358, USA
Manuscript submitted May 30, 2024, accepted June 15, 2024, published online June 25, 2024
Short title: Anomalous Origin of LVA Associated With Left SSS
doi: https://doi.org/10.14740/cr1672
| Abstract | ▴Top |
The subclavian steal syndrome (SSS) is defined by the reversal of flow in the ipsilateral vertebral artery in the setting of subclavian artery stenosis proximal to its origin. Here, we describe a rare case of left SSS with significant left subclavian artery stenosis associated with anomalous origin of the left vertebral artery (LVA) directly from the aortic arch in a patient presenting with signs of vertebrobasilar insufficiency and resolution of symptoms following angioplasty. Through this case, the authors try to emphasize the importance and the correct technique of using Doppler ultrasonography, and the importance of invasive angiography in understanding the mechanism of subclavian steal in patients with anomalous LVA origin.
Keywords: Subclavian steal syndrome; Subclavian artery stenosis; Anomalous origin of the left Vertebral artery; Vascular anomalies
| Introduction | ▴Top |
Subclavian steal syndrome (SSS) is a condition associated with the reversal of blood flow in the ipsilateral vertebral artery due to hemodynamically significant stenosis or occlusion of the ipsilateral proximal subclavian artery (PSCA) [1]. While most of the patients with the underlying condition remain asymptomatic, they can present with symptoms of vertebrobasilar insufficiency (VBI) and upper extremity ischemia [2]. The atherosclerotic disease remains the most common etiology [2]. Here, we describe a rare case of left-sided SSS in a patient with anomalous left vertebral artery (LVA) origin directly from the aortic arch with a reported incidence of 2.4-5.8% [3]. A detailed understanding of the vertebral arteries’ origin is paramount due to advanced endovascular diagnostic imaging and surgical interventions available today. Computed tomography angiography (CTA) or magnetic resonance angiography (MRA) are the confirmatory tests that define the anatomy of the subclavian stenosis or occlusion and other associated vascular abnormalities [1]. Doppler ultrasonography is of specific importance as it can detect the presence of retrograde vertebral flow in cases of SSS [1]. Vascular interventions are only indicated in symptomatic patients, and angioplasty with stent placement remains the gold standard therapeutic approach [4, 5]. Through this case, the authors emphasize the importance of meticulous investigation while evaluating SSS and that the anomalous origin of LVA directly from the aortic arch can still be implicated in VBI.
| Case Report | ▴Top |
Investigations
A 71-year-old male with a history of nicotine dependence, hypertension, hyperlipidemia, type 2 diabetes mellitus, chronic obstructive lung disease (COPD), and atrial fibrillation presented to the emergency department (ED) for worsening dizziness, especially while moving his left arm. The dizziness was not associated with any left arm pain or fatigue with exertion. Other reviews of systems were unremarkable and the patient was hemodynamically stable on presentation. The physical examination findings were unremarkable.
Diagnosis
The basic laboratory workup was unremarkable. The initial carotid duplex showed no significant internal carotid artery (ICA) stenosis and normal antegrade flow in both vertebral arteries (Fig. 1). However, 45 mm Hg of the pressure difference between the two arms prompted a dedicated left upper arm arterial duplex, which suggested hemodynamically significant left subclavian artery (LSCA) stenosis and flow reversal in the LVA (Fig. 1) when it was scanned/imaged higher up in the neck. CTA of neck arteries confirmed 90% stenosis of the proximal LSCA and interestingly showed the LVA originated from the aortic arch between the left common carotid artery (LCCA) and LSCA (Fig. 2). Invasive LVA angiography confirmed anomalous origin and showed collaterals from the mid-distal vertebral artery supplying blood flow to the left arm distal to stenosis via the thyrocervical trunk (Figs. 3 and 4).
 Click for large image | Figure 1. (a) Carotid artery duplex showing normal anterograde flow in the left vertebral artery. (b) Monophasic waveform suggesting left subclavian artery stenosis. (c) Reversal of flow in the left vertebral artery when imaged higher up in the neck. |
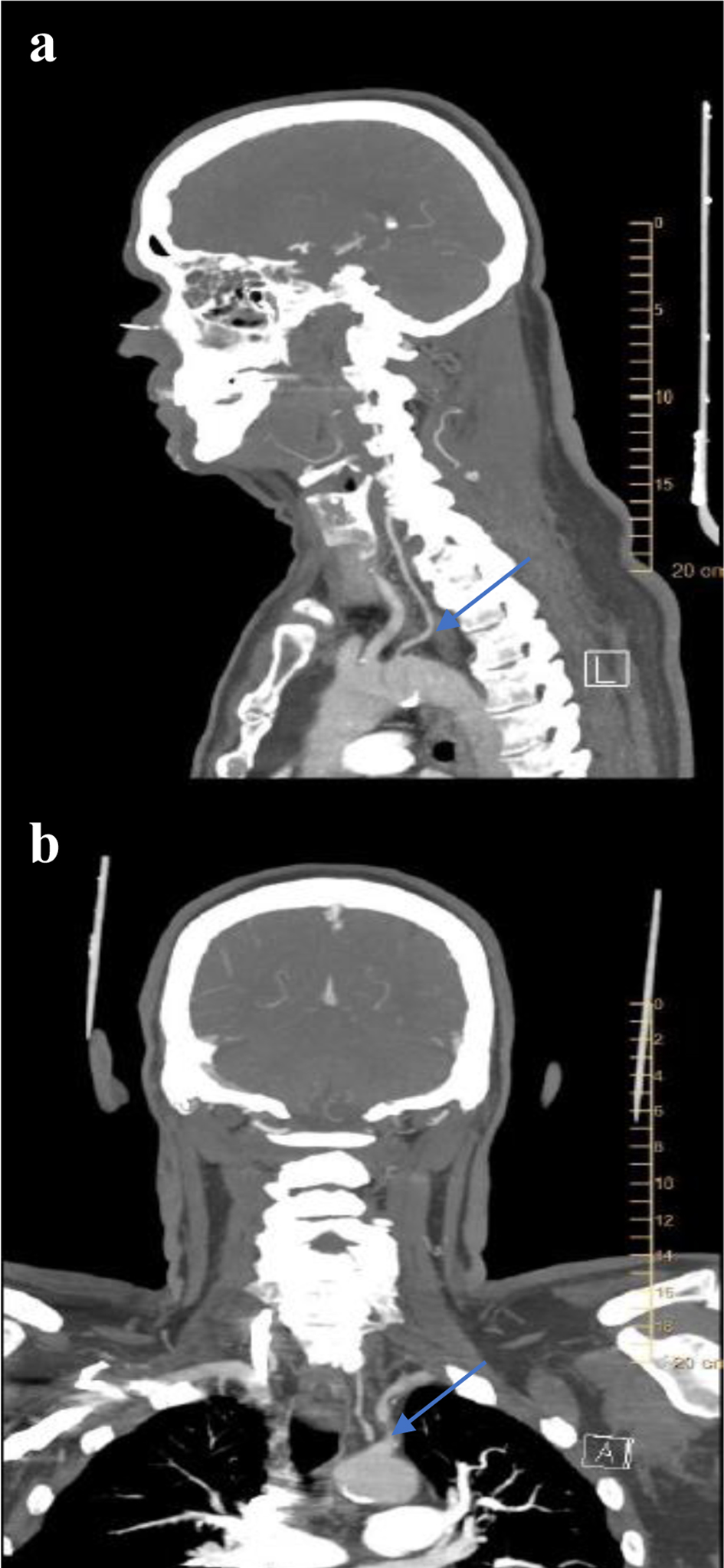 Click for large image | Figure 2. CT angiogram of neck showing (a) the anomalous origin of the left vertebral artery directly from the aortic arch between the left common carotid artery and the left subclavian artery (LSCA) (blue arrow), and (b) proximal LSCA stenosis (blue arrow). |
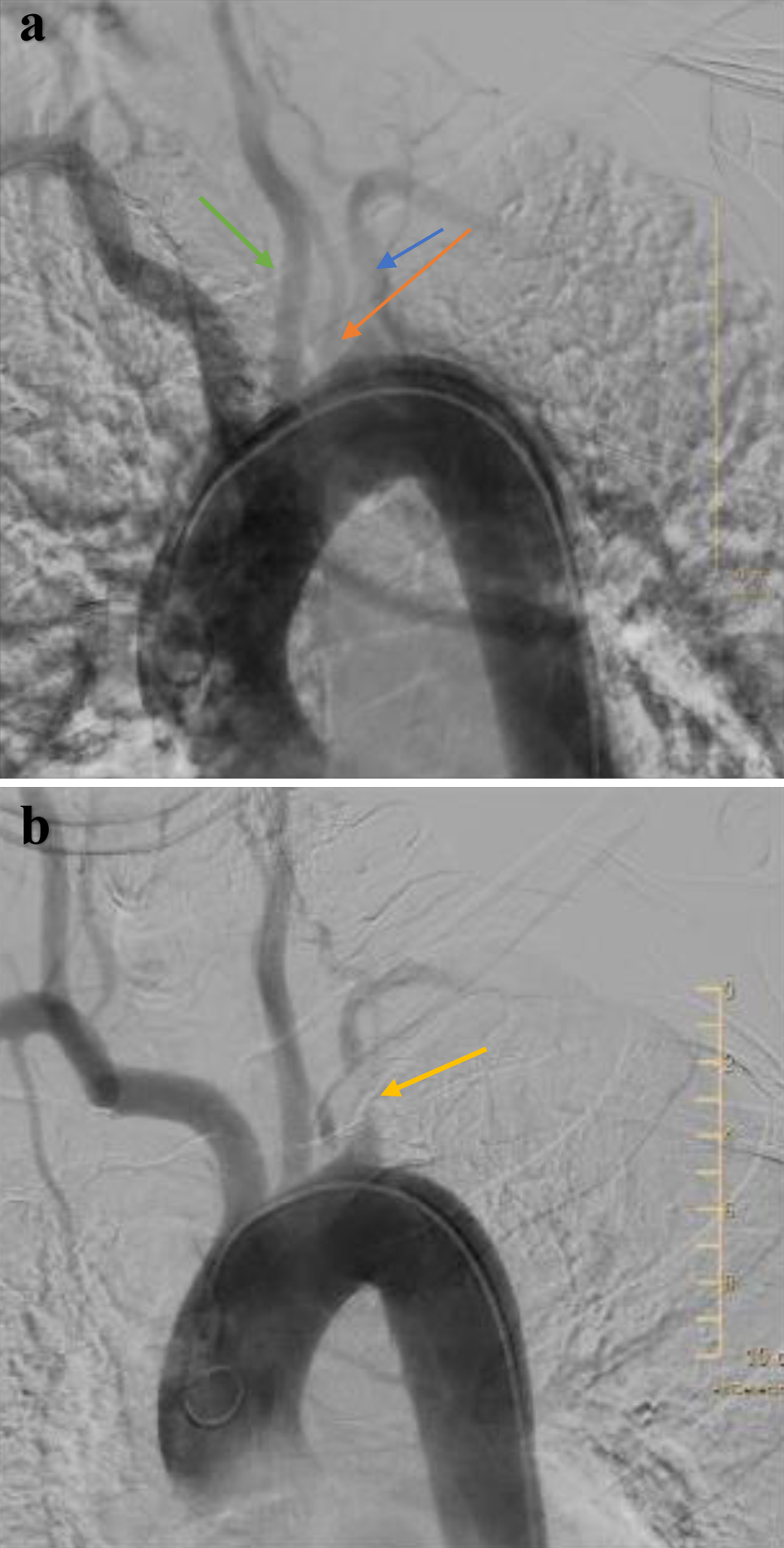 Click for large image | Figure 3. Aortic arch angiogram showing (a) the anomalous origin of the left vertebral artery (orange arrow) directly from the aortic arch between the left common carotid artery (green arrow) and the left subclavian artery (LSCA) (blue arrow), and (b) proximal LSCA stenosis. |
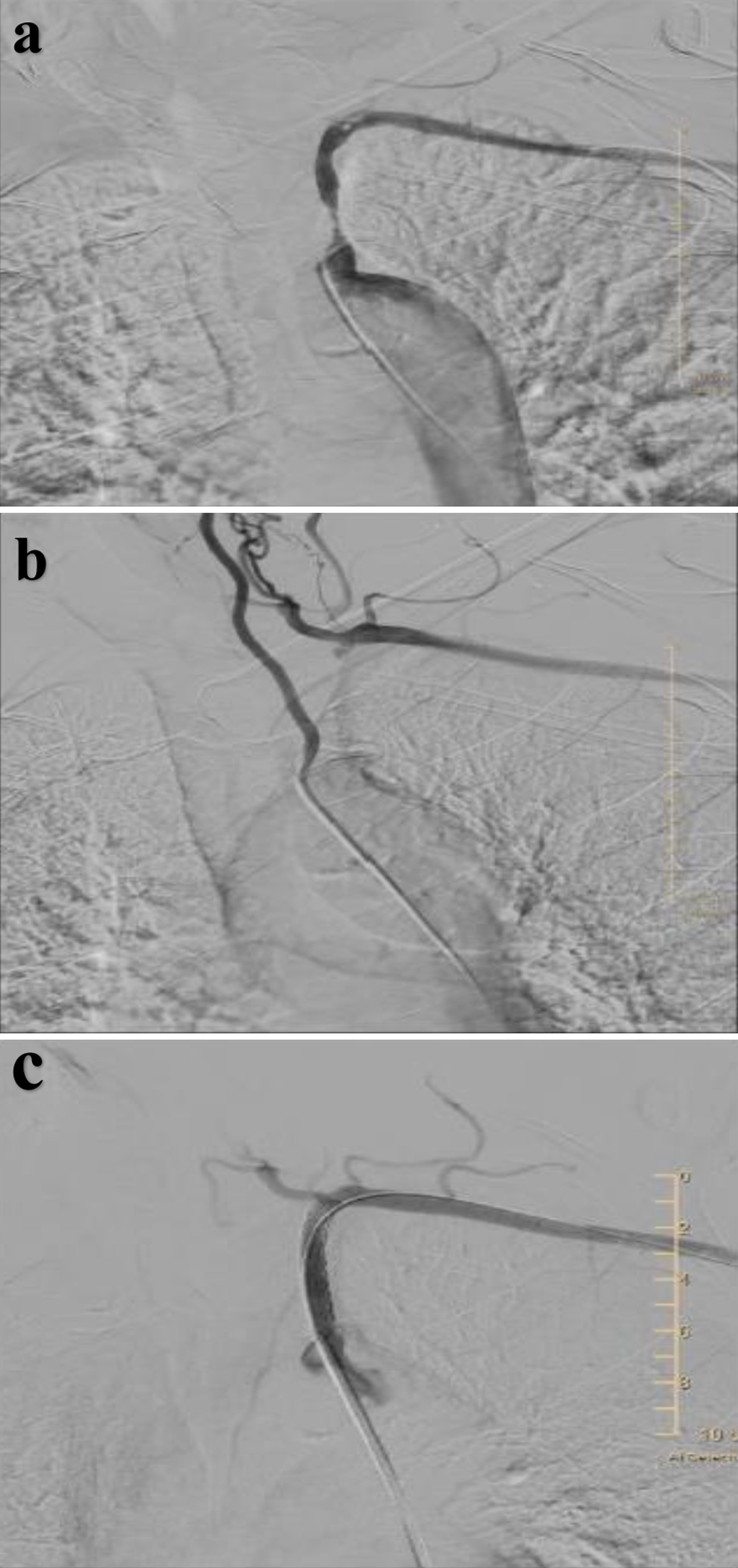 Click for large image | Figure 4. (a) Selective angiography confirming significant stenosis of the proximal left subclavian artery (LSCA) with no flow in thyrocervical trunk, (b) selective angiography of left vertebral artery showing retrograde flow in the collaterals from mid-distal vertebral artery to LSCA distal to the stenosis via the thyrocervical trunk, and (c) left subclavian artery (after stent placement in proximal segment) now showing antegrade flow in the thyrocervical trunk. |
Treatment
The LSCA stenosis was treated with a balloon expandable covered stent placement, and the final angiogram showed antegrade flow in thyrocervical trunk networks. Patients’ dizziness significantly improved on follow-up.
Follow-up
The patient was discharged home with outpatient follow-up with cardiology and vascular surgery in 4 - 6 weeks.
| Discussion | ▴Top |
SSS is a condition associated with the reversal of blood flow in the ipsilateral vertebral artery due to hemodynamically significant stenosis or occlusion of the ipsilateral PSCA [1, 2]. The incidence and prevalence of SSS are not very well defined due to asymptomatic presentation [6]. The studies have shown the incidence of subclavian artery occlusion of 17% and 9% of them were symptomatic [6]. The atherosclerotic disease remains the most common etiology; however, other conditions to consider include thoracic outlet syndrome, cervical rib, Takayasu arteritis, and stenosis due to surgical repair of coarctation of aorta or tetralogy of Fallot [2]. The risk factors for SSS include smoking, hypertension, hyperlipidemia, diabetes mellitus, family history, and age [1]. While most of the patients with the underlying condition remain asymptomatic, they can present with symptoms of VBI (dizziness while moving left arm), upper extremity claudication, or cardiac angina [2]. Symptomatic SSS presentation is more often seen in males over 50 years of age with a 2:1 male-to-female ratio [1, 6].
The branching patterns of the aortic arch were studied by Popieluszko et al, in the meta-analysis of 23,882 adult aortic arches from 51 studies which showed that the most common branching pattern (from right to left), brachiocephalic trunk, the LCCA, and the LSCA with an overall incidence of 80.9% [7]. The second most common pattern was the bovine arch variant in 13.6%, where the aortic arch gives off only two main branches, followed by the left vertebral artery variant in 2.8% where the aortic arch gives off four main branches (from right to left), brachiocephalic trunk, the LCCA, the LVA, and the LSCA [7]. Although asymptomatic in most cases, this anomalous origin of the LVA has been associated with arterial aneurysm, atherosclerotic disease-causing stroke, and aortic dissection [5, 8]. However, anomalous LVA origin directly from the aortic arch can be associated with left SSS as seen in our patient.
Embryonically, the anomalous origin of the LVA directly from the aortic arch is due to the overabsorption of embryonic tissue of the LSCA and is more seen in females [7, 8]. In most cases of the anomalous origin of the LVA, patients are asymptomatic; however, there is a statistically significant association between the presence of a vertebral artery that originates directly from the aortic arch and Stanford B aortic dissection [5]. The straight-through origin of the vertebral artery from the arch may result in increased flow in the posterior circulation/circle of Willis and could be a risk factor for cerebrovascular diseases including thrombosis, aneurysm, arterial dissection, and atherosclerotic disease [9]. A detailed understanding of the origin of the vertebral arteries is of paramount importance due to advanced endovascular diagnostic imaging and surgical interventions available today.
Duplex ultrasound (DUS) is the mainstay of diagnosis wherein it can show a flow reversal in LVA when there is ipsilateral PSCA stenosis [9]. However, the initial DUS in our patient did not show flow reversal in LVA since the LVA was scanned in its proximal segment (closer to its origin) where the flow will be antegrade. CTA or MRA are the confirmatory tests that define the anatomy of subclavian stenosis or occlusion and can detect the presence of other associated vascular abnormalities [1]. Our patient did have CTA which showed severe stenosis of left PSCA, but interestingly showed anomalous LVA origin directly from the aortic arch. So, we questioned as to why our patient would have VBI symptoms. This was answered by an invasive angiogram which showed the thyrocervical branches stealing blood from a mid-distal segment of LVA and supplying blood to the left arm beyond LSCA stenosis. This explains why the second DUS in our patient showed flow reversal in LVA since it was scanned higher up in the neck.
According to an observational study by Labropoulos et al, 7,881 carotid duplex scans were performed over 6 years and SSS was complete in 61% and partial in 23% of patients [10]. Symptoms were present in only 38 patients and only seven underwent intervention (five with percutaneous transluminal angioplasty stenting of the subclavian and two with subclavian-carotid bypass) [10]. A significantly elevated pressure differential (PD) between two arms of > 50 mm Hg was associated with symptoms, complete steal, and need for intervention [10]. All patients with SSS are not candidates for vascular intervention. Conservative management includes treating hypertension, diabetes mellitus, and smoking cessation with close outpatient monitoring using ultrasound [10]. In cases of isolated subclavian steno-occlusive disease, carotid-subclavian bypass surgery is known to have high patency rates at 95% at 10 years with no mortality with 8 years of follow-up [11, 12]. However, with evolving cutting-edge technology, endovascular therapy has been shown to have similar clinical outcomes compared to open surgery with minimal risks [4]. According to Wang et al, a success rate of 95.1% is achieved with angioplasty and stenting, and a 12-month follow-up primary patency rate was 98% [13]. Our patient did undergo angioplasty following which showed improvement in his symptoms.
Conclusion
Left SSS in patients with anomalous origin of the LVA directly from the aortic arch is due to the stealing of blood via an extensive collateral network of vessels connecting the vertebral artery to the thyrocervical trunk. In such case, blood flow at the origin of the LVA will be in an antegrade direction contrary to that usually reported in this condition, unless the LVA is imaged higher up in the neck.
Learning points
SSS is often underdiagnosed, and it is crucial to perform a good physical examination to recognize the difference in blood pressure between bilateral upper extremities and confirm reversal of flow using the Doppler ultrasonography.
SSS can be associated with other vascular anomalies like the anomalous origin of the LVA directly from the aortic arch, wherein the steal happens through thyrocervical collaterals connecting the LVA and the LSCA.
Doppler ultrasonography should incorporate scanning the LVA both proximally and distally to look for a flow reversal in patients with high clinical suspicion of SSS.
Acknowledgments
None to declare.
Financial Disclosure
No grants, contracts, or other forms of financial support are involved in the work.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained from the patient.
Author Contributions
Poornima Vinod: writing the original draft, including the literature search, review, and editing. Hiten Patel: supervision, review, and editing.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Osiro S, Zurada A, Gielecki J, Shoja MM, Tubbs RS, Loukas M. A review of subclavian steal syndrome with clinical correlation. Med Sci Monit. 2012;18(5):RA57-RA63.
doi pubmed pmc - Potter BJ, Pinto DS. Subclavian steal syndrome. Circulation. 2014;129(22):2320-2323.
doi pubmed - Newton TH, Mani RH. The vertebral artery. In: Newton H, Potts DG, editors. Radiology of the skull and brain, anatomy and pathology. St. Louis: Mosby; 1977. p. 1659-1707.
- Galkin PV, Antonov GI, Mitroshin GE, Terekhin SA, Bobkov Iu A. [Surgical correction of cerebral blood flow steal syndrome by aortic branches stenosis]. Khirurgiia (Mosk). 2009;7:15-21.
pubmed - Tapia GP, Zhu X, Xu J, Liang P, Su G, Liu H, Liu Y, et al. Incidence of branching patterns variations of the arch in aortic dissection in Chinese patients. Medicine (Baltimore). 2015;94(17):e795.
doi pubmed pmc - Leach DF, 3rd, Radwanski DM, Kaur P, Das DD, Kondapalli M. Recurrent subclavian steal syndrome: a novel case of vasculopathy. Cureus. 2023;15(1):e33310.
doi pubmed pmc - Onrat E, Uluisik IE, Ortug G. The left vertebral artery arising directly from the aortic arch. Transl Res Anat. 2021;24:100122.
- Nayak SR, Pai MM, Prabhu LV, D’Costa S, Shetty P. Anatomical organization of aortic arch variations in the India: embryological basis and review. J Vasc Bras. 2006;5:95-100.
doi - Satti SR, Cerniglia CA, Koenigsberg RA. Cervical vertebral artery variations: an anatomic study. AJNR Am J Neuroradiol. 2007;28(5):976-980.
pubmed pmc - Labropoulos N, Nandivada P, Bekelis K. Prevalence and impact of the subclavian steal syndrome. Ann Surg. 2010;252(1):166-170.
doi pubmed - Uurto IT, Lautamatti V, Zeitlin R, Salenius JP. Long-term outcome of surgical revascularization of supra-aortic vessels. World J Surg. 2002;26:1503.
- AbuRahma AF, Robinson PA, Jennings TG. Carotid-subclavian bypass grafting with polytetrafluoroethylene grafts for symptomatic subclavian artery stenosis or occlusion: a 20-year experience. J Vasc Surg. 2000;32(3):411-418; discussion 418-419.
doi pubmed - Wang KQ, Wang ZG, Yang BZ, Yuan C, Zhang WD, Yuan B, Xing T, et al. Long-term results of endovascular therapy for proximal subclavian arterial obstructive lesions. Chin Med J (Engl). 2010;123(1):45-50.
pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.