

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 4, August 2024, pages 253-261

Usefulness of Serum Testosterone Concentration and Skin Autofluorescence as Coronary Risk Markers in Male Patients With Type 2 Diabetes Mellitus
Takashi Hitsumoto
Hitsumoto Medical Clinic, Shimonoseki City, Yamaguchi 750-0025, Japan
Manuscript submitted June 18, 2024, accepted July 15, 2024, published online July 30, 2024
Short title: Testosterone and Skin AF in Male T2DM
doi: https://doi.org/10.14740/cr1686
| Abstract | ▴Top |
Background: No studies have reported simultaneous evaluation of the two coronary risk markers of testosterone and skin autofluorescence (SAF) as a marker of advanced glycation end products in patients with type 2 diabetes mellitus (T2DM) at present. This study aimed to clarify the clinical significance of both indicators as risk markers of coronary artery disease (CAD), including the association and background factors between testosterone and SAF in male patients with T2DM.
Methods: This study enrolled 162 male patients with T2DM (CAD: n = 35). Testosterone was evaluated by serum total testosterone concentration (T-T). Various analyses related to T-T and SAF as coronary risk markers were performed.
Results: T-T was significantly lower, and SAF was significantly higher in patients with CAD than in patients with non-CAD. A significant negative correlation was found between T-T and SAF (r = -0.45, P < 0.001), and the correlation was stronger in patients with CAD than in patients with non-CAD (non-CAD, r = -0.27, P = 0.003; CAD, r = -0.51, P < 0.001). However, both T-T and SAF had significant associations with triglyceride-glucose index as an insulin resistance marker and cardio-ankle vascular index as an arterial function marker. Multiple regression analysis revealed that both T-T and SAF were selected as independent variables to the presence of CAD as a dependent variable. However, the odds ratio increased due to the merger of two coronary risk markers, low T-T and high SAF (odds ratio: one risk marker: 3.24, 95% confidence interval: 1.01 - 10.50, P = 0.045; two risk markers: 13.22, 95% confidence interval: 3.41 - 39.92, P < 0.001).
Conclusions: The results of this cross-sectional study indicate that T-T and SAF are closely related in CAD patients with T2DM. It also shows that insulin resistance and arterial dysfunction are in the background of both indicators. Additionally, not only are both indicators independent coronary risk markers, but the overlap of both indicators increases their weight as coronary risk markers.
Keywords: Testosterone; Skin autofluorescence; Type 2 diabetes mellitus; Male; Coronary artery disease; Triglyceride-glucose index; Cardio-ankle vascular index
| Introduction | ▴Top |
Type 2 diabetes mellitus (T2DM) is no doubt one of the major coronary risk factors [1], and patients with coronary artery disease (CAD) complicated by T2DM are encountered in daily practice. However, comprehensive therapeutic interventions, including blood glucose levels and classical coronary risk factors, significantly reduced the incidence of CAD, but the residual risk still exists in patients with T2DM [2]. Therefore, exploring novel coronary risk markers other than blood glucose levels and classical coronary risk markers in patients with T2DM is clinically meaningful with the aim of further reducing risk.
Testosterone is known as an important sex hormone produced in the testes that maintain male health. Additionally, researchers in the basic and clinical fields have shown that low testosterone affects arteriosclerosis progression [3-5]. However, several reports have been presented in recent years that have clarified the importance of low blood testosterone concentration as a coronary risk factor in male patients with T2DM [6, 7]. Therefore, measuring blood testosterone concentration in male patients with T2DM and intervening therapeutically are expected to prevent the onset of CAD.
Several researchers have emphasized the importance of advanced glycation end products (AGEs) in arteriosclerosis progression [8-10]. However, medical devices that noninvasively measure and evaluate the accumulation of AGEs under the skin of the examinee’s forearm have been developed and clinically applied in recent years [11]. Clinical researchers have shown that elevated skin autofluorescence (SAF) measured by the device is closely related to arteriosclerosis progression [12-14]. Additionally, recent clinical studies have revealed a significant relationship between coronary arteriosclerosis and SAF in patients with T2DM [15, 16].
Therefore, low blood testosterone in males and elevated SAF are considered notable coronary risk markers in patients with T2DM; however, to date, no study has reported a combined evaluation of their clinical significance as a coronary risk marker, including the relationship between these two indicators in male patients with T2DM. This study aimed to clarify the clinical significance of both indicators as coronary risk markers, including the association and background factors between testosterone and SAF in male patients with T2DM.
| Materials and Methods | ▴Top |
Patients
Among the outpatient men with T2DM who presented to Hitsumoto Medical Clinic between December 2021 and November 2023, 162 consecutive patients with all clinical parameters, including blood testosterone levels and SAF, were enrolled. Blood testosterone concentration was evaluated by serum total testosterone concentration (T-T) using a commercial kit (ARCHITECT Estradiol II, Chicago, IL, USA), and SAF was measured using a commercial device (AGE reader mu; DiagnOptics, Groningen, the Netherlands). Various analyses related to T-T and SAF were performed.
Ethical considerations
The clinical study complied with the ethical principles of the Declaration of Helsinki, which is the ethical principle of medical research involving human beings. Informed consent was obtained from all study participants, and the Institutional Review Board of Hitsumoto Medical Clinic approved the study protocol (date of approval: November 15, 2021; approval number: HMC-2021-12R-2).
The evaluation of clinical parameters
Various clinical parameters, such as age, glucose-related indicators, smoking habits, blood pressure levels, serum lipid levels, history of CAD, inflammation, kidney function, and cardio-ankle vascular index (CAVI), were evaluated. The degree of obesity was evaluated by body mass index. Smokers were defined based on the description in the medical record and had a smoking habit within the observation period of this study. The definition of CAD in this study was defined as patients who underwent coronary revascularization for angina pectoris and/or myocardial infarction, judged from the description in the medical record or the interview. Blood samples were collected from peripheral veins using a standard method while fasting, and blood glucose-related indicators, lipid-related indicators, inflammation, and kidney function indicators were evaluated. Triglyceride-glucose (TyG) index was calculated as a marker of insulin resistance by a previous report (Ln (fasting serum triglyceride levels (mg/dL) × fasting blood glucose levels (mg/dL)/2)) [17]. Serum high-sensitivity C-reactive protein concentration (hs-CRP) was measured as an inflammatory marker. The estimated glomerular filtration rate (eGFR) was calculated using a Japanese report as a marker of kidney function [18]. CAVI was measured using a VaSera CAVI instrument (Fukuda Denshi, Tokyo, Japan) as a marker of arterial function following the previously described methods [19, 20]. Oral medications, such as biguanide, dipeptidyl peptidase-4 inhibitor, sulfonylurea, thiazolidinedione, sodium-glucose cotransporter 2 inhibitor, and statin, were evaluated, as well as exogenous insulin use.
Statistical analysis
The commercialized software MedCalc for Windows (MedCalc Software, Ostend, Belgium) and Stat View-J version 5.0 (HULINKS Inc., Tokyo, Japan) was used for the statistical analysis. Continuous variables were expressed as means and standard deviations or medians (interquartile range). The unpaired t-test or Mann-Whitney U test was used to perform comparisons between groups. Simple regression analysis was performed using Pearson’s correlation coefficient or Spearman rank correlation. Receiver operating characteristic curves were created to decide the optimal cut-off point of T-T or SAF for the presence of CAD. Multivariate analysis was performed using multiple regression analysis or multiple logistic regression analysis. Multiple regression analysis was performed for CAD as a dependent variable. The selection of explanatory factors was determined by considering the multicollinearity of factors significantly associated with CAD and factors significantly associated with T-T and SAF, and 10 factors (age, hemoglobin A1c, TyG index, serum low-density lipoprotein cholesterol (LDL-C) levels, hs-CRP, eGFR, CAVI, T-T, SAF, statin use) were selected. P values of < 0.05 were considered statistically significant.
| Results | ▴Top |
Background of patients with and without CAD
Background factors for patients with and without CAD are shown in Table 1. A history of CAD was found in 35 patients. There were 18 cases (11%) that met the diagnostic criteria for hypotestosteronemia in Japan (T-T level less than 250 ng/dL). Patients with CAD had significantly higher statin usage and significantly lower serum total cholesterol concentration and serum LDL-C concentration than those with non-CAD. Age, TyG index, serum triglyceride concentration, hs-CRP, and CAVI were significantly higher, but eGFR was significantly lower in patients with CAD than in those without. However, T-T was significantly lower (non-CAD vs. CAD, 520.5 ± 149.9 ng/dL vs. 341.8 ± 161.1 ng/dL, P < 0.001), and SAF was significantly higher (non-CAD vs. CAD, 2.7 ± 0.5 arbitrary unit vs. 3.4 ± 0.5 arbitrary unit, P < 0.001) in patients with CAD than in those without.
 Click to view | Table 1. Clinical Characteristics of the Studied Groups |
Correlation between T-T and SAF
Figure 1 shows a correlation between T-T and SAF. A significantly negative correlation was found between T-T and SAF in all study groups (r = -0.45, P < 0.001). However, the correlation was stronger in patients with CAD than in those without, according to the correlation with the presence or absence of CAD (non-CAD, r = -0.27, P = 0.003; CAD, r = -0.51, P < 0.001).
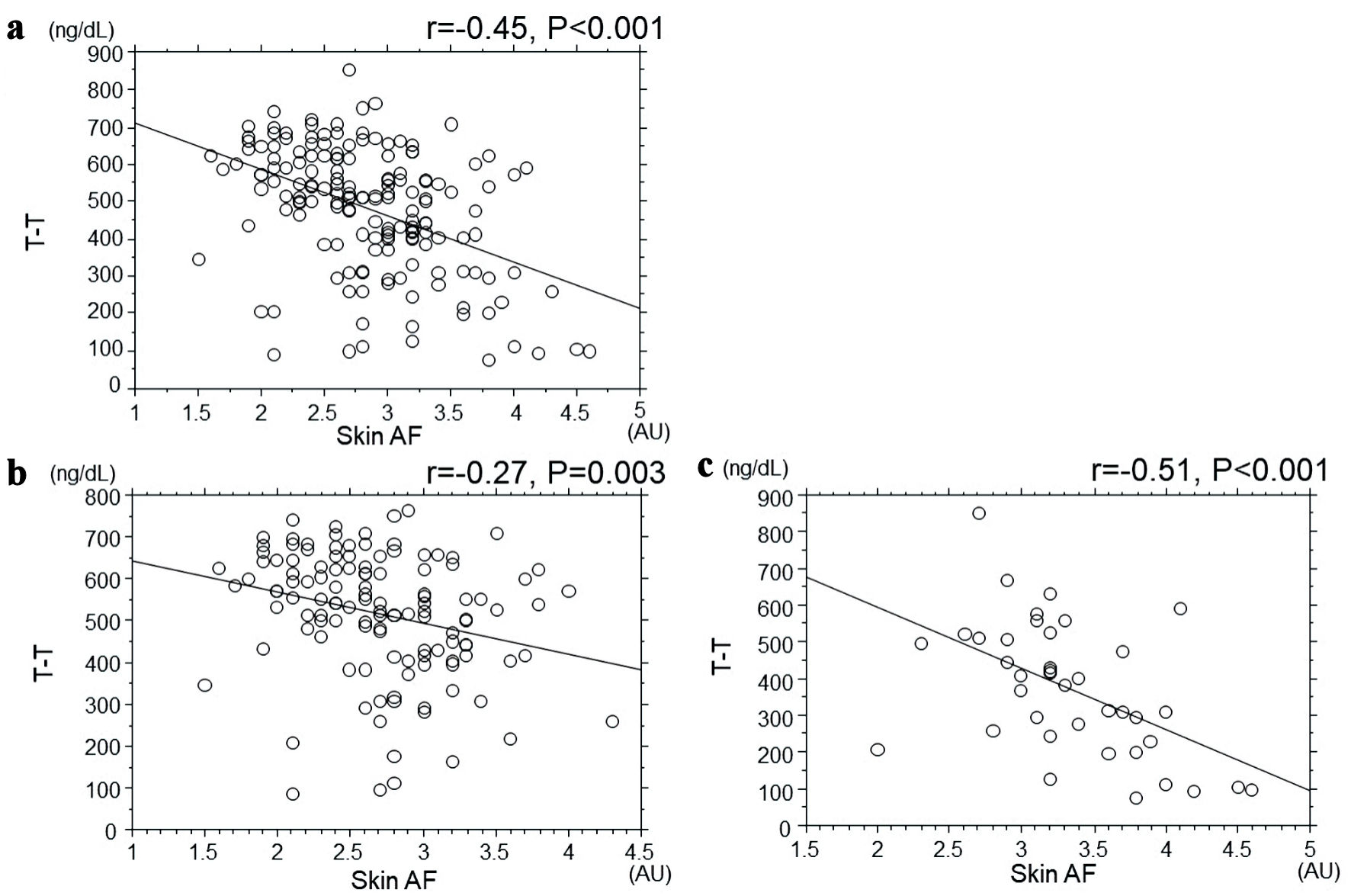 Click for large image | Figure 1. Correlation between T-T and SAF. (a) All patients. (b) Non-CAD patients. (c) CAD patients. There was a significant negative correlation between T-T and SAF in all study groups ((a) r = -0.45, P < 0.001). However, as a result of examining the correlation with the presence or absence of CAD, the correlation was stronger in CAD patients than in non-CAD patients ((b) non-CAD: r = -0.27, P = 0.003; (c) CAD: r = -0.51, P < 0.001). T-T: total testosterone; SAF: skin autofluorescence; CAD: coronary artery disease; AU: arbitrary unit. |
Correlations between T-T, SAF, and various clinical parameters
Table 2 shows the correlation between T-T, SAF and various clinical parameters. T-T had significantly negative correlations with age, fasting blood glucose levels, hemoglobin A1c, TyG index, serum triglyceride concentration, hs-CRP, and CAVI. However, T-T had a significantly positive correlation with eGFR. SAF had significantly positive correlations with age, smoking habits, fasting blood glucose levels, hemoglobin A1c, TyG index, serum triglyceride concentration, hs-CRP, and CAVI. However, SAF had a significantly negative correlation with eGFR and sodium-glucose cotransporter 2 inhibitor use.
Click to view | Table 2. Correlation Between T-T, SAF and Various Clinical Parameters |
Multiple regression analysis for CAD
The results of multiple regression analysis for CAD are shown in Table 3. Five factors (LDL-C, CAVI, SAF, T-T, and TyG index) were selected as independent variables to CAD as a dependent variable.
Click to view | Table 3. Multiple Regression Analysis for CAD |
CAD risks due to the combination of T-T and SAF
Figure 2 shows the study results on CAD risks by combining T-T and SAF. The optimal cut-off values for detecting CAD based on receiver operating characteristic curve analysis were 474.5 ng/dL for T-T and 3.0 arbitrary unit for SAF. However, the odds ratio (OR) significantly increased by combining the low T-T with the high SAF (OR: one risk marker: 3.24, 95% confidence interval: 1.01 - 10.50, P = 0.045; two risk markers: 13.22, 95% confidence interval: 3.41 - 39.92, P < 0.001).
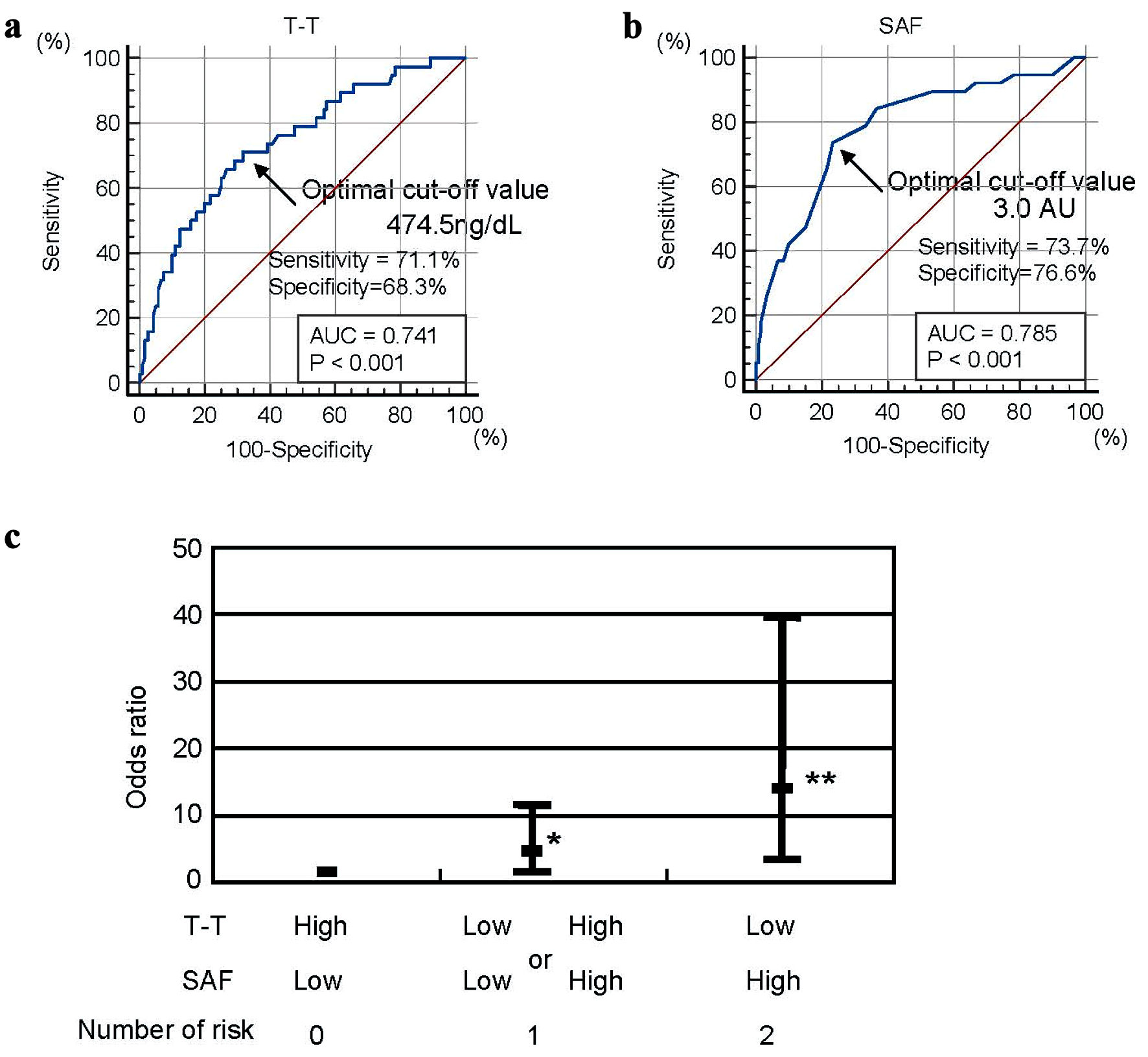 Click for large image | Figure 2. CAD risks due to the combination of T-T and SAF. The optimal cut-off values for detecting CAD based on receiver operating characteristic curve analysis were 474.5 ng/dL for T-T (a), and 3.0 AU for SAF (b). However, the OR significantly increased by combining the low T-T with the high SAF (c) (OR: one risk marker: 3.24, 95% CI: 1.01 - 10.50, P = 0.045; two risk markers: 13.22, 95% CI: 3.41 - 39.92, P < 0.001) The analysis was corrected by the LDL-C, CAVI, TyG index, and age, and the bar expressed 95% CI. *P = 0.039, **P < 0.001. CAD: coronary artery disease; T-T: total testosterone; SAF: skin autofluorescence; OR: odds ratio; CI: confidence interval; AU: arbitrary unit; AUC: area under the curve; LDL-C: low-density lipoprotein cholesterol; CAVI: cardio-ankle vascular index; TyG: triglyceride-glucose. |
| Discussion | ▴Top |
This study aimed to clarify the clinical significance of both indicators as coronary risk markers, including the association and background factors of T-T and SAF in male patients with T2DM. Multiple regression analysis revealed that decreased LDL-C levels were selected as the strongest variable to CAD as a subordinate factor, this may be due to the active use of statins to reduce LDL-C levels in CAD patients compared to non-CAD patients for the prevention of coronary secondary events. However, as in previous reports, in the results of this study, T-T were significantly lower, and SAF were significantly higher in patients with CAD than in those without. In addition, a significantly negative correlation was found between T-T and SAF, and the correlation was stronger in patients with CAD than in those without. T-T and SAF were significantly correlated with the TyG index, which is an insulin resistance indicator, and CAVI, which is an arterial function indicator, respectively; and the TyG index and CAVI were also selected as independent variables to the presence of CAD as the subordinate factor. Additionally, not only were low T-T and high SAF each selected as independent variables for CAD as a dependent factor, but OR were significantly increased by assessing both measures at the same time.
Relationships between testosterone and AGEs
Several basic research results have been reported showing an association between testosterone and AGEs. Qi et al reported that AGEs inhibit Leydig cell production in rats [21]. Additionally, Zhao et al show that oxidative stress and endoplasmic reticulum stress are involved in inhibiting testosterone production by AGEs [22]. Therefore, the mechanism of AGEs suppressing testosterone production in testicular has a possibility to cause the significant negative association between T-T and SAF obtained in this study. However, study results indicate a stronger association between T-T and SAF in patients with CAD than in those without. Therefore, testosterone and AGEs are closely related in the coronary arteries and cause the development of coronary atherosclerotic lesions. A study by Xie et al using human umbilical endothelial cells reported that testosterone within the physiological range ameliorates disorders caused by AGEs [23]. Therefore, lower testosterone and elevated AGEs cause coronary endothelial dysfunction with each other, indicating its contribution to a significant association between the two indices in patients with CAD in this study. Several researchers have focused on the importance of chronic low inflammation levels in the progression of coronary atherosclerotic lesions [24, 25]. Study results revealed that hs-CRP, which is an inflammation indicator, was significantly higher in patients with CAD than in those without although with no significant factor in the multiple regression analysis. Additionally, both T-T and SAF were significantly related to hs-CRP in univariate analysis. However, several researchers have revealed a close relationship between low testosterone or high AGEs and inflammation in coronary artery vessels [26, 27]. Therefore, inflammation may be involved in the background of the negative correlation between T-T and SAF in patients with CAD. Basic and clinical studies on the relationship between testosterone and AGEs focusing on coronary arteries and inflammation are hoped to be conducted in the future to clarify this issue.
Testosterone, SAF, and TyG index
Several researchers have pointed out that insulin resistance plays an important role in arteriosclerosis development [28, 29]. Additionally, the TyG index, which is an indicator of insulin resistance, is recently reported to be significantly associated with patients with T2DM with CAD [30, 31]. This result is consistent with the results obtained in this study. However, this study revealed a significant association between the TyG index for both T-T and SAF. Several researchers have confirmed a significant association between the TyG index and lower blood testosterone levels in male patients with T2DM, similar to the study results [32, 33]. However, to the author’s knowledge, this is the first study to investigate the relationship between SAF and the TyG index in male patients with T2DM. Follow-up studies are hoped to be conducted on the relationship between SAF and the TyG index, including intervention trials.
Testosterone, SAF, and CAVI
CAVI is not only an indicator of systemic arterial stiffness [19], but also reflects vascular endothelial function in patients with T2DM [34] and is attracting attention as a new arteriosclerosis indicator. Additionally, several reports of high CAVI levels have been reported in patients with T2DM with CAD [35, 36], which is consistent with the study results. However, both T-T and SAF were significantly related to CAVI in this study. In addition, existing reports have shown an association between arterial stiffness and hypotestosteronemia or high SAF, supporting the validity of the findings [37, 38]. This study focused on CAD, but existing reports emphasized that CAVI is associated with arteriosclerotic lesion progressions throughout the body, such as cerebrovascular disease, heart failure, and kidney disease [39-41]. Further, from this point of view, T-T and SAF are considered contributors not only to the development of CAD but also to various arteriosclerosis-related diseases through vascular insufficiency in male patients with T2DM. Therefore, additional research related to various arteriosclerosis diseases focusing on two indicators, including T-T and SAF in male patients with T2DM, are hoped to be conducted in the future.
Usefulness of simultaneous measurement evaluation of T-T and SAF
The cut-off values of T-T and SAF (T-T: 474.5 ng/dL, SAF: 3.0 arbitrary unit) specified by CAD were determined by receiver operating characteristic curves to evaluate the usefulness of simultaneous measurement evaluation of T-T and SAF in this study, and multiple logistic regressions analysis determined the overlapping weight of these two indicators to CAD. The result revealed increased OR to CAD due to the overlap of these two indicators. This is not a prospective study but a cross-sectional study, and therapeutic interventions based on the required cut-off values, which are expected to prevent the onset of CAD events in male patients with T2DM in daily practice, despite related limitations. However, both T-T and SAF are related to lifestyle [20, 42-44], indicating that active lifestyle modifications for male patients with T2DM having these two indicators may be important in addition to management, such as blood glucose and LDL-C reduction for CAD event prevention.
Limitations
The limitations of this study are described below. First, many patients with non-CAD were not evaluated for coronary artery stenosis using coronary angiography or coronary computed tomography angiography. Existing reports indicate that asymptomatic patients with diabetes have 30.5% of cases of significant coronary stenosis using coronary computed tomography angiography [45]. Therefore, it cannot be ruled out that cases with asymptomatic coronary artery stenosis are included in patients with non-CAD, and thus, caution should be exercised in the result interpretation. Second, this was a cross-sectional study conducted at a single institution in Japan, and the number of cases is relatively small. It is necessary to consider whether the same results will be achieved in other races. Furthermore, prospectively verifying the usefulness of combined evaluation of T-T and SAF in male patients with T2DM using a larger number of cases from multiple institutions, including intervention trials such as testosterone replacement therapy and AGEs-lowering therapy, is desirable in the future.
Conclusions
The results of this cross-sectional study indicate that T-T and SAF are closely related in CAD patients with T2DM. It also shows that insulin resistance and arterial dysfunction are in the background of both indicators. Additionally, not only are both indicators independent coronary risk markers, but the overlap of both indicators increases their weight as coronary risk markers. Large prospective studies that include intervention therapies are required to validate the study results.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained from all patients who participated in this study.
Author Contributions
Takashi Hitsumoto contributed to the research planning, data acquisition and analysis, and manuscript writing and editing.
Data Availability
The author declares that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Booth GL, Kapral MK, Fung K, Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet. 2006;368(9529):29-36.
doi pubmed - Ueki K, Sasako T, Okazaki Y, Kato M, Okahata S, Katsuyama H, Haraguchi M, et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951-964.
doi pubmed - Hotta Y, Kataoka T, Kimura K. Testosterone deficiency and endothelial dysfunction: nitric oxide, asymmetric dimethylarginine, and endothelial progenitor cells. Sex Med Rev. 2019;7(4):661-668.
doi pubmed - Akishita M, Hashimoto M, Ohike Y, Ogawa S, Iijima K, Eto M, Ouchi Y. Low testosterone level is an independent determinant of endothelial dysfunction in men. Hypertens Res. 2007;30(11):1029-1034.
doi pubmed - Hitsumoto T. Clinical significance of low blood testosterone concentration in men as a cardiovascular risk factor from the perspective of blood rheology. Cardiol Res. 2019;10(2):106-113.
doi pubmed pmc - Madhu SV, Aslam M, Aiman AJ, Siddiqui A, Dwivedi S. Prevalence of hypogonadism in male Type 2 diabetes mellitus patients with and without coronary artery disease. Indian J Endocrinol Metab. 2017;21(1):31-37.
doi pubmed pmc - Saluja M, Galav V, Pillai D, Chittora S. Low serum testosterone levels in male patients with type 2 diabetes mellitus as a risk factor for coronary artery disease. J Assoc Physicians India. 2021;69(9):11-12.
pubmed - Ren X, Ren L, Wei Q, Shao H, Chen L, Liu N. Advanced glycation end-products decreases expression of endothelial nitric oxide synthase through oxidative stress in human coronary artery endothelial cells. Cardiovasc Diabetol. 2017;16(1):52.
doi pubmed pmc - Xing Y, Pan S, Zhu L, Cui Q, Tang Z, Liu Z, Liu F. Advanced glycation end products induce atherosclerosis via RAGE/TLR4 signaling mediated-M1 macrophage polarization-dependent vascular smooth muscle cell phenotypic conversion. Oxid Med Cell Longev. 2022;2022:9763377.
doi pubmed pmc - Singh S, Siva BV, Ravichandiran V. Advanced Glycation End Products: key player of the pathogenesis of atherosclerosis. Glycoconj J. 2022;39(4):547-563.
doi pubmed - Meerwaldt R, Links TP, Graaff R, Hoogenberg K, Lefrandt JD, Baynes JW, Gans RO, et al. Increased accumulation of skin advanced glycation end-products precedes and correlates with clinical manifestation of diabetic neuropathy. Diabetologia. 2005;48(8):1637-1644.
doi pubmed - van Eupen MG, Schram MT, van Sloten TT, Scheijen J, Sep SJ, van der Kallen CJ, Dagnelie PC, et al. Skin autofluorescence and pentosidine are associated with aortic stiffening: the maastricht study. Hypertension. 2016;68(4):956-963.
doi pubmed - Hitsumoto T. Relationships Between Arterial Pressure-Volume Index and Cardiovascular Disease Biomarkers in Patients With Hypertension. J Clin Med Res. 2022;14(6):229-236.
doi pubmed pmc - Osawa S, Katakami N, Kuroda A, Takahara M, Sakamoto F, Kawamori D, Matsuoka T, et al. Skin autofluorescence is associated with early-stage atherosclerosis in patients with type 1 diabetes. J Atheroscler Thromb. 2017;24(3):312-326.
doi pubmed pmc - Hangai M, Takebe N, Honma H, Sasaki A, Chida A, Nakano R, Togashi H, et al. Association of advanced glycation end products with coronary artery calcification in japanese subjects with type 2 diabetes as assessed by skin autofluorescence. J Atheroscler Thromb. 2016;23(10):1178-1187.
doi pubmed pmc - Planas A, Simo-Servat O, Baneras J, Sanchez M, Garcia E, Ortiz AM, Ruiz-Meana M, et al. Usefulness of skin advanced glycation end products to predict coronary artery calcium score in patients with type 2 diabetes. Acta Diabetol. 2021;58(10):1403-1412.
doi pubmed - Simental-Mendia LE, Rodriguez-Moran M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299-304.
doi pubmed - Imai E, Horio M, Nitta K, Yamagata K, Iseki K, Hara S, Ura N, et al. Estimation of glomerular filtration rate by the MDRD study equation modified for Japanese patients with chronic kidney disease. Clin Exp Nephrol. 2007;11(1):41-50.
doi pubmed - Shirai K, Utino J, Otsuka K, Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J Atheroscler Thromb. 2006;13(2):101-107.
doi pubmed - Hitsumoto T. Relationships between skin autofluorescence and cardio-ankle vascular index in japanese male patients with metabolic syndrome. Cardiol Res. 2019;10(3):172-180.
doi pubmed pmc - Qi YW, Hu CY, Chen SH, Liu Y. Advanced glycation end products inhibit testosterone secretion by rat Leydig cells by inducing oxidative stress and endoplasmic reticulum stress. Zhonghua Nan Ke Xue. 2014;20(5):410-413.
- Zhao YT, Qi YW, Hu CY, Chen SH, Liu Y. Advanced glycation end products inhibit testosterone secretion by rat Leydig cells by inducing oxidative stress and endoplasmic reticulum stress. Int J Mol Med. 2016;38(2):659-665.
doi pubmed - Xie Y, Yu D, Wu J, Li L. Protective effects of physiological testosterone on advanced glycation end product-induced injury in human endothelial cells. Mol Med Rep. 2017;15(3):1165-1171.
doi pubmed pmc - Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685-1695.
doi pubmed - Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation. 2005;111(25):3481-3488.
doi pubmed - Malkin CJ, Pugh PJ, Jones RD, Jones TH, Channer KS. Testosterone as a protective factor against atherosclerosis—immunomodulation and influence upon plaque development and stability. J Endocrinol. 2003;178(3):373-380.
doi pubmed - Wang X, Xu T, Mungun D, Zhou C, Zha Z, Lu M, Fen C, et al. The relationship between plasma soluble receptor for advanced glycation end products and coronary artery disease. Dis Markers. 2019;2019:4528382.
doi pubmed pmc - Howard G, O'Leary DH, Zaccaro D, Haffner S, Rewers M, Hamman R, Selby JV, et al. Insulin sensitivity and atherosclerosis. The insulin resistance atherosclerosis study (IRAS) investigators. Circulation. 1996;93(10):1809-1817.
doi pubmed - Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011;14(5):575-585.
doi pubmed pmc - Si Y, Fan W, Shan W, Zhang Y, Liu J, Han C, Sun L. Association between triglyceride glucose index and coronary artery disease with type 2 diabetes mellitus in middle-aged and elderly people. Medicine (Baltimore). 2021;100(9):e25025.
doi pubmed pmc - Thai PV, Tien HA, Van Minh H, Valensi P. Triglyceride glucose index for the detection of asymptomatic coronary artery stenosis in patients with type 2 diabetes. Cardiovasc Diabetol. 2020;19(1):137.
doi pubmed pmc - Caretta N, Facondo P, Mereu S, Delbarba A, Crepaldi MC, Vedovato M, Avogaro A, et al. Cardiometabolic indices predict hypogonadism in male patients with type 2 diabetes. J Endocrinol Invest. 2023;46(3):599-608.
doi pubmed pmc - Yu Y, Wang Y, Xu L, Li W, Wang Y. Combined obesity- and lipid-related indices are associated with hypogonadism in Chinese male patients with type 2 diabetes: a cross-sectional study. Front Endocrinol (Lausanne). 2023;14:1319582.
doi pubmed pmc - Endo K, Saiki A, Ohira M, Miyashita Y, Shirai K. Cardio-ankle vascular index may reflect endothelial function in type 2 diabetes. Int J Clin Pract. 2011;65(11):1200-1201.
doi pubmed - Mineoka Y, Fukui M, Tanaka M, Tomiyasu K, Akabame S, Nakano K, Yamazaki M, et al. Relationship between cardio-ankle vascular index (CAVI) and coronary artery calcification (CAC) in patients with type 2 diabetes mellitus. Heart Vessels. 2012;27(2):160-165.
doi pubmed - Niwa H, Takahashi K, Dannoura M, Oomori K, Miyoshi A, Inada T, Miyoshi H. The association of cardio-ankle vascular index and ankle-brachial index with macroangiopathy in patients with type 2 diabetes mellitus. J Atheroscler Thromb. 2019;26(7):616-623.
doi pubmed pmc - Hougaku H, Fleg JL, Najjar SS, Lakatta EG, Harman SM, Blackman MR, Metter EJ. Relationship between androgenic hormones and arterial stiffness, based on longitudinal hormone measurements. Am J Physiol Endocrinol Metab. 2006;290(2):E234-242.
doi pubmed - Birukov A, Cuadrat R, Polemiti E, Eichelmann F, Schulze MB. Advanced glycation end-products, measured as skin autofluorescence, associate with vascular stiffness in diabetic, pre-diabetic and normoglycemic individuals: a cross-sectional study. Cardiovasc Diabetol. 2021;20(1):110.
doi pubmed pmc - Choi SY, Park HE, Seo H, Kim M, Cho SH, Oh BH. Arterial stiffness using cardio-ankle vascular index reflects cerebral small vessel disease in healthy young and middle aged subjects. J Atheroscler Thromb. 2013;20(2):178-185.
doi pubmed - Hitsumoto T. Efficacy of the reactive oxygen metabolite test as a predictor of initial heart failure hospitalization in elderly patients with chronic heart failure. Cardiol Res. 2018;9(3):153-160.
doi pubmed pmc - Zhang C, Zhong Y, Tian H. Increased cardio-ankle vascular index is independently associated with chronic kidney disease: A cross-sectional study in Chinese patients with type 2 diabetes mellitus. J Diabetes Complications. 2019;33(9):623-627.
doi pubmed - Devi S, Saxena J, Rastogi D, Goel A, Saha S. Effect of short-term physical exercise on serum total testosterone levels in young adults. Indian J Physiol Pharmacol. 2014;58(2):178-181.
pubmed - Maiorino MI, Bellastella G, Esposito K. Lifestyle modifications and erectile dysfunction: what can be expected? Asian J Androl. 2015;17(1):5-10.
doi pubmed pmc - van Waateringe RP, Slagter SN, van der Klauw MM, van Vliet-Ostaptchouk JV, Graaff R, Paterson AD, Lutgers HL, et al. Lifestyle and clinical determinants of skin autofluorescence in a population-based cohort study. Eur J Clin Invest. 2016;46(5):481-490.
doi pubmed pmc - Kamimura M, Moroi M, Isobe M, Hiroe M. Role of coronary CT angiography in asymptomatic patients with type 2 diabetes mellitus. Int Heart J. 2012;53(1):23-28.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.