

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 4, August 2024, pages 275-280

Patients With ST-Segment Elevation Myocardial Infarction and Cerebrovascular Accidents: Impact of COVID-19 Vaccination on Mortality
Sharvil Patela, f, Mahmoud Ballouta, Sandus Khana, Shane Robinsonb, Alex M. Adamsc, Ania Rynarzewskad, John E. Delzell Jre
aInternal Medicine Department, Northeast Georgia Medical Center, Gainesville, GA, USA
bGME Research, Northeast Georgia Medical Center, Gainesville, GA, USA
cCardiology Department, Northeast Georgia Medical Center, Gainesville, GA, USA
dGME Research, Georgia College and State University, Milledgeville, GA, USA
eDepartment of Graduate Medical Education, Northeast Georgia Medical Center, Gainesville, GA, USA
fCorresponding Author: Sharvil Patel, Internal Medicine Department, Northeast Georgia Medical Center, Gainesville, GA 30501, USA
Manuscript submitted June 20, 2024, accepted August 2, 2024, published online August 20, 2024
Short title: COVID-19 Vaccine and STEMI/CVA Mortality
doi: https://doi.org/10.14740/cr1688
| Abstract | ▴Top |
Background: Coronavirus disease 2019 (COVID-19) infection is associated with proinflammatory states and adverse health outcomes such as ST-segment elevation myocardial infarction (STEMI) and cerebrovascular accidents (CVA). Limited evidence suggests that COVID-19 vaccination may decrease the adverse impact of COVID-19 infections. This study was designed to determine if patients who received COVID-19 vaccination had lower mortality from STEMI and CVA.
Methods: This is a retrospective comparative analysis of 3,050 patients, who were admitted to the hospital and diagnosed with STEMI or CVA between April 1, 2019, and April 1, 2022. Patients were divided into three different timeframes: pre-COVID (April 1, 2019, to March 31, 2020), COVID (April 1, 2020 to March 31, 2021), and post-COVID (April 1, 2021 to March 31, 2022). Chi-square analysis was completed to analyze associations between STEMI, CVA, and vaccination status. A multinominal logistic regression was used to determine significant predictors for in-hospital mortality.
Results: A total of 3,050 patients were admitted (1,873 STEMI and 1,177 CVA). STEMI accounted for about 60% of cases in each of the three time periods. There was no statistical difference in STEMI or CVA percentages in the three time periods. There was increased mortality in STEMI and CVA patients (odds ratio (OR) = 11.4; P < 0.001), but patients who received the COVID-19 vaccine were less likely to die (OR = 0.51, 95% confidence interval (CI): 0.28 - 0.93; P < 0.027) when compared to those who were unvaccinated. There was increased risk of death in patients with atrial fibrillation (AFIB) (OR = 2.43; P < 0.001) and chronic heart failure (CHF) (OR = 1.76; P = 0.004). There was increased mortality risk associated with age (OR =1.03; P = 0.001). Patients with coronary artery disease (CAD) (OR = 0.45; P = 0.014) and hyperlipidemia (OR = 0.29; P < 0.001) were less likely to die.
Conclusions: Vaccination against COVID-19 was associated with reduced mortality rates in patients hospitalized with STEMI and CVA. Patients with pre-existing cardiovascular comorbidities such as CAD and hyperlipidemia also had lower mortality.
Keywords: COVID-19 vaccination; Mortality; STEMI; CVA
| Introduction | ▴Top |
The global pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), commonly known as coronavirus disease 2019 (COVID-19), affected more than 675 million people [1]. There is an increased risk of complications such as acute myocardial infarction (AMI) and cerebrovascular accident (CVA) associated with COVID-19 infection [2]. Most complications happen in patients with comorbidities that affect the cardiovascular and pulmonary system [3]. The hypothesized mechanism of endothelial dysfunction with apoptosis is direct viral infection of the angiotensin-converting enzyme 2 (ACE2) receptor expressed on endothelial cells, resulting in activation of the immune system, affecting multiple different organs [3]. A meta- analysis in 2021 found higher in-hospital mortality in patients with a STEMI who had COVID-19 infection versus those with no infection [4]. A meta-analysis from 2020 found that patients with COVID-19 and concurrent cardiovascular disease, hypertension, diabetes, congestive heart failure, and chronic kidney disease had a greater risk of mortality compared to patients without these comorbidities [5]. A systematic review in 2021 found patients with COVID-19 infection and stroke had higher in-hospital mortality [6].
Three vaccines for the prevention of COVID-19 infection were developed and approved in the United States. More than 13.3 billion COVID vaccines have been administered since the beginning of the pandemic [7]. With global efforts, 70.6% of the world’s population has now received at least one dose of COVID-19 vaccine [7]. Studies have shown an association between COVID-19 and proinflammatory states, which leads to ST-segment elevation myocardial infarction (STEMI) and CVA; however, there is less evidence that vaccine administration impacts the outcomes of STEMI and CVA in COVID-19 patients [2]. A study in Korea in 2022 found that full vaccination was associated with decreased risk of AMI and ischemic stroke in patients with COVID-19 infection [8]. There are no prior studies of the influence of vaccination status on hospital outcomes. Therefore, the purpose of this retrospective study is to assess the relationship between COVID-19 vaccination status and mortality and prevalence of STEMI and CVA in patients with multiple underlying cardiovascular comorbidities.
| Materials and Methods | ▴Top |
Subjects
All patients admitted to Northeast Georgia Health System from April 1, 2019, to March 31, 2022, with a diagnosis of STEMI or CVA were included in this retrospective observational study. The study used deidentified secondary data. Data acquisition was completed using ethical data governance to maintain anonymity of the patients involved in the study. This study was granted exemption from full Institutional Review Board (IRB) review by the IRB at the Brenau University. The investigation conforms with the principles outlined in the Declaration of Helsinki.
Design
A retrospective observational study was performed with patients admitted to one of four hospitals in a medium-sized health system between April 1, 2019, and March 31, 2022. Patients admitted with a primary diagnosis of STEMI or CVA were included. Data were collected through chart abstraction from electronic health records using the Current Procedural Terminology (CPT) and International Classification of Diseases, 10th Revision (ICD-10) codes. The date of these encounters was used to divide patients into three groups to observe the relationship between COVID-19 and the onset of CVAs and STEMIs. The patients were divided into times before, during, and after the COVID-19 pandemic (Fig. 1). The control group (pre-COVID) was patients admitted in the year immediately prior to the beginning of the COVID-19 pandemic dated from April 1, 2019, to March 31, 2020. The pre-COVID group functions to record the annual baseline occurrence of CVAs and STEMIs prior to the COVID-19 pandemic. The second group (COVID) included patients admitted from April 1, 2020, to March 31, 2021. The third group was after the introduction of COVID vaccination. The post-COVID group included patients admitted from April 1, 2021, to March 31, 2022. Patients were considered “vaccinated” if they had received two doses of the COVID-19 vaccine, regardless of the specific vaccine received. Figure 1 outlines the group allocation. To clarify the role that COVID-19 infection and vaccination status have on the outcomes of CVA and stroke, additional data on cardiovascular and metabolic comorbidities - including coronary artery disease (CAD), atrial fibrillation (AFIB), type 2 diabetes mellitus (T2DM), hyperlipidemia, chronic heart failure (CHF), along with patient demographics were collected.
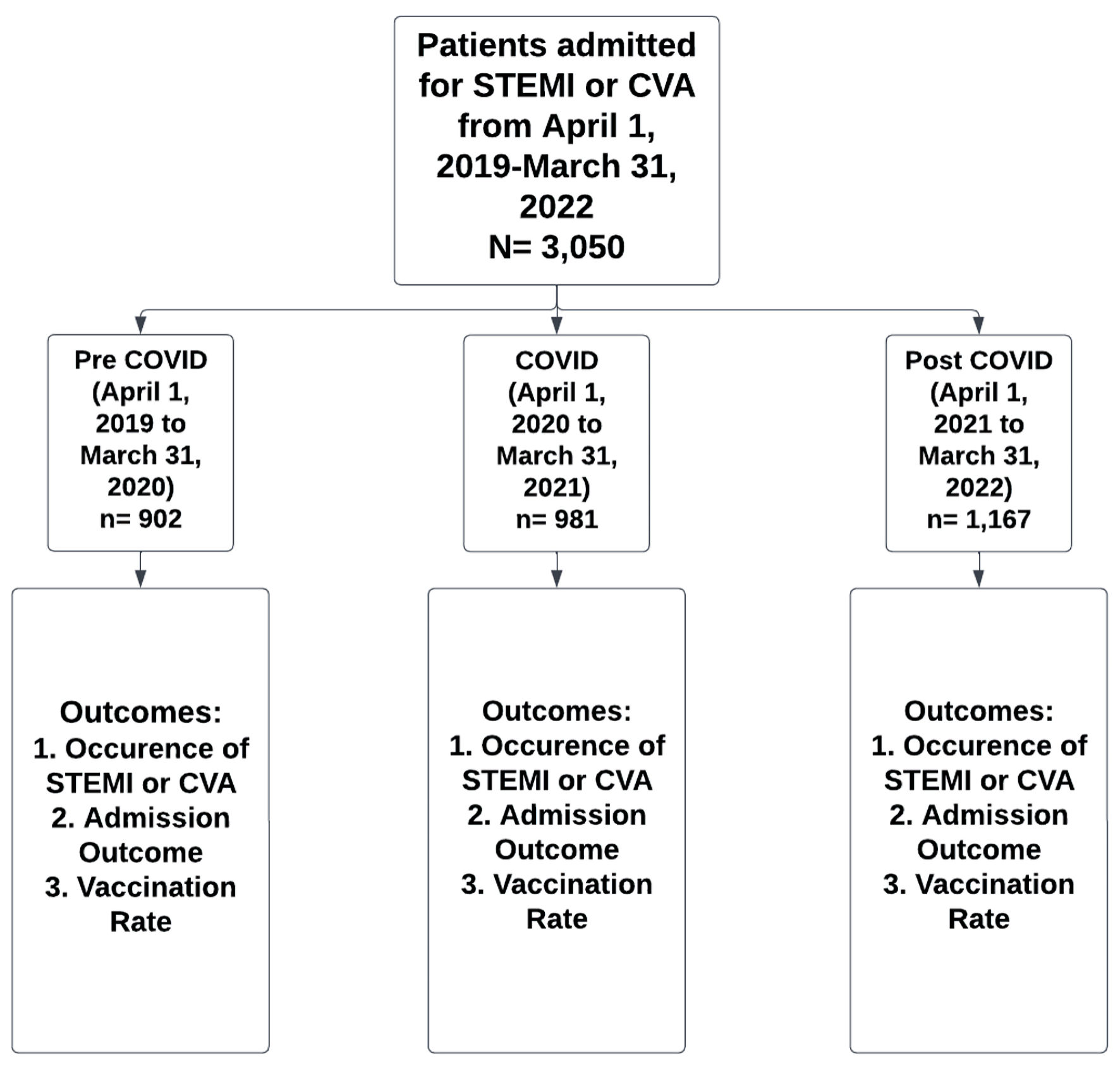 Click for large image | Figure 1. Group allocation and study design. STEMI: ST-segment elevation myocardial infarction; CVA: cerebrovascular accident; COVID-19: coronavirus disease 2019. |
Outcomes
The primary outcome was mortality in patients presenting with STEMI and CVA before, during, and after the COVID-19 pandemic. COVID-19 vaccination status was recorded as present or absent. Patient characteristics and comorbidities were included to determine if there were any predictors for mortality or confounders.
Statistical analysis
Nonparametric data of the prevalence of STEMI and CVAs and COVID vaccination status by COVID-19 group year was analyzed using Chi-square to determine COVID group associations with STEMI and/or CVA. To determine the relationship between COVID-19 vaccination and mortality, a multinomial logistic regression analysis was conducted. The model was used to determine if any variables (CVA or STEMI, COVID vaccination, COVID-19, age, CAD, AFIB, hyperlipidemia, CHF, COVID group year, and T2DM) could significantly predict mortality in patients presenting with a primary diagnosis of STEMI or CVA. All statistical analyses were performed using IBM SPSS 28.0 with an alpha level of 0.05 to determine significance for all statistical tests.
| Results | ▴Top |
Prevalence of STEMI and CVA
During the study time period, a total of 3,050 patients were admitted (1,873 with a STEMI and 1,177 with a CVA). STEMI accounted for about 60% of cases in each time period. In contrast, stroke constituted approximately 40% of cases across the three COVID groups. Neither CVAs nor STEMIs were statistically associated with COVID-related time frames, but there were increases in both STEMIs and CVAs in the post-COVID-19 group compared to both pre-COVID-19 and COVID-19 groups (Table 1).
 Click to view | Table 1. Occurrence of STEMI and CVA Events per Group Year |
COVID-19 vaccination rates
There was a significant association between the COVID groups and vaccination rates. COVID-19 vaccination became available in December of 2021. Seventeen patients in the COVID timeframe were vaccinated. In the post-COVID group, slightly over four in 10 patients (44.9%) received a COVID vaccine (Table 2).
Click to view | Table 2. Vaccination Rates of Patients Admitted With STEMI or CVA |
Prediction for in-hospital mortality
STEMI and CVA patients have an increased risk of death (odds ratio (OR) = 11.4, 95% confidence interval (CI): 6.1 - 21.5; P < 0.001). Patients who received COVID vaccine were less likely to die (OR = 0.51, 95% CI: 0.28 - 0.93; P < 0.027). Patients with CAD (OR = 0.45, 95% CI: 0.233 - 0.847; P = 0.014) and hyperlipidemia (OR = 0.29, 95% CI: 0.192 - 0.434; P < 0.001) were also less likely to die. There was increased risk of death in patients with AFIB (OR = 2.43, 95% CI: 1.632 - 3.611; P < 0.001) and CHF (OR = 1.76; 95% CI: 1.195 - 2.60; P = 0.004). There was an increased mortality risk associated with age (OR =1.03, 95% CI: 1.017 - 1.049). T2DM was not a significant predictor for mortality but remains in the model (Table 3).
Click to view | Table 3. Predictors for In-Hospital Mortality |
| Discussion | ▴Top |
Pre-existing cardiovascular, pulmonary, and metabolic diseases are consistently associated with severe COVID-19 infection and worse long-term outcomes. COVID-19 vaccination was introduced to decrease the spread of COVID infection and was found to decrease the severity of illness. The purpose of this study was to determine if there was a relationship between COVID-19 vaccination and outcomes of hospitalizations relating to STEMI or CVA. This study found that patients who were diagnosed with COVID-19 infection had increased mortality from STEMI and CVA; however, those who received two doses of the COVID-19 vaccination had a decreased mortality risk. STEMI and CVA prevalence were not associated with COVID-related timeframes.
This study indicates that STEMI and CVA patients who were hospitalized at our institution and were considered completely vaccinated had a lower mortality rate. These findings are consistent with previous literature showing the cardioprotective effects of COVID-19 vaccination on cardiovascular outcomes. A study by Gupta et al found a significant reduction in all-cause mortality in vaccinated patients with AMI at 30 days and 6-month follow-up [9]. Kim et al found that full vaccination against COVID-19 was associated with a reduced risk of AMI and ischemic stroke after COVID-19 infection [8]. Our results confirmed these findings even in consideration of patients who suffered from pre-existing cardiovascular comorbidities, such as CAD and hyperlipidemia. This further emphasizes that individuals with pre-existing cardiovascular disease should be vaccinated in order to improve cardiovascular outcomes. Data regarding the protective effects of COVID-19 on cardiovascular events are still limited, and further research should be conducted.
Zahid et al found that STEMI patients with superimposed COVID-19 infection had worse clinical outcomes, with almost three times higher in-hospital mortality and a higher rate of 6-month major adverse cardiac events [10]. Other diagnoses that were predictors for mortality in these patients were AFIB, CHF, and post-COVID syndrome. COVID-19 vaccination is valuable for all patients, but patients with these diagnoses should prioritize vaccination. COVID-19 predisposes patients to arterial and venous thrombosis due to excessive inflammation, platelet activation, endothelial dysfunction, and stasis [11, 12]. Furthermore, studies have shown that COVID-19 induces multiple cytokines and chemokines resulting in vascular inflammation, plaque instability, and myocardial inflammation [13].
In this study, STEMI and CVA prevalence were not significantly different pre-COVID versus during and after COVID. Data from the United States National COVID Cohort Collaborative reported that both full and partial vaccination against COVID-19 were associated with decreased risk of major adverse cardiac events [14]. In our population, only 44.9% of the patients had received a COVID vaccination in the post-COVID period. This may be linked to vaccine hesitancy. Jabagi et al evaluated patients over 75 years old from France who had received COVID vaccination. They found no increase in the risk of stroke, acute MI, and pulmonary embolism in the first 14 days after vaccination [15]. Lin et al reviewed patients from North Carolina who received COVID vaccination and found lower risk of subsequent COVID infection, hospitalization, and death [16].
As a retrospective observational design, this study cannot establish causation or direct correlation. Additionally, the small cohort size in this study compared to the general population of vaccinated individuals may mask significant findings and lead to potential confounders. Presentation bias is another limitation that can be considered, as many patients with cardiovascular events might have developed a fear of going to the hospital during the peak of COVID. Furthermore, this study did not account for the potential effect of long-COVID syndrome on cardiovascular disease outcomes. Data regarding anticoagulation status were not reported in this study, as it is known that aspirin has a cardioprotective profile. The role of thromboprophylaxis after diagnosis of COVID was not investigated and could have altered outcomes on mortality of STEMI and CVA patients. This study did not account for the specific type of vaccination given. Patients were considered “vaccinated” if they received two doses of the vaccine which excludes patients with one dose. Finally, we were unable to account for modification in STEMI and CVA management for those who were COVID-19 positive, such as delayed percutaneous coronary intervention (PCI), thrombectomy, or limited imaging to decrease staff exposure to COVID-19.
Despite knowing that COVID-19 vaccination is beneficial in reducing mortality with STEMI and CVA, the exact mechanism as to how COVID-19 vaccination reduces the severity of these cardiovascular events remains unclear. While COVID vaccination is strongly encouraged for all populations, patients that experience specific comorbidities like AFIB and CHF should prioritize vaccination. Further research needs to be done to explore the impact of COVID-19 vaccination on these higher-risk populations and how long-COVID affects cardiovascular health. This will help better spread awareness to decrease vaccine hesitancy for optimal recovery and prevention of COVID, and its related consequences.
Acknowledgments
We would like to thank the Graduate Medical Education research team from Northeast Georgia Medical Center for supporting this research study.
Financial Disclosure
This study did not receive any funding.
Conflict of Interest
The authors declare there is no conflict of interest.
Informed Consent
This is a retrospective study that reviewed secondary data. Therefore, the IRB waved the need for informed consent for the participants involved in the study.
Author Contributions
SP, MB, and SK were responsible for data collection, manuscript writing, and the development of background and methodology of the study in its origination. JD assisted as the faculty sponsor of the project with reviewing and editing of the entire manuscript and helped with clinical interpretations of data analysis. SR was responsible as the methodologist of the project and assisted in ethical compliance with IRB submission and review. AR served as the statistician of the study and worked with data cleaning, organization, and analysis. AA and JD conceived the original idea and were responsible for supervising the project.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Hamimes A, Lounis M, Aouissi HA, Roufayel R, Lakehal A, Bouzekri H, Byeon H, et al. The role of vaccination and face mask wearing on COVID-19 infection and hospitalization: a cross-sectional study of the MENA region. Healthcare (Basel). 2023;11(9):1257.
doi pubmed pmc - Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. 2022;28(3):583-590.
doi pubmed pmc - Oliveira RKF, Nyasulu PS, Iqbal AA, Hamdan Gul M, Ferreira EVM, Leclair JW, Htun ZM, et al. Cardiopulmonary disease as sequelae of long-term COVID-19: Current perspectives and challenges. Front Med (Lausanne). 2022;9:1041236.
doi pubmed pmc - Thakker RA, Elbadawi A, Chatila KF, Goel SS, Reynoso D, Berbarie RF, Gilani S, et al. Comparison of coronary artery involvement and mortality in STEMI patients with and without SARS-CoV-2 during the COVID-19 pandemic: a systematic review and meta-analysis. Curr Probl Cardiol. 2022;47(3):101032.
doi pubmed pmc - Ssentongo P, Ssentongo AE, Heilbrunn ES, Ba DM, Chinchilli VM. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. PLoS One. 2020;15(8):e0238215.
doi pubmed pmc - Nannoni S, de Groot R, Bell S, Markus HS. Stroke in COVID-19: A systematic review and meta-analysis. Int J Stroke. 2021;16(2):137-149.
doi pubmed pmc - Hasell J, Mathieu E, Beltekian D, Macdonald B, Giattino C, Ortiz-Ospina E, Roser M, et al. A cross-country database of COVID-19 testing. Sci Data. 2020;7(1):345.
doi pubmed pmc - Kim YE, Huh K, Park YJ, Peck KR, Jung J. Association between vaccination and acute myocardial infarction and ischemic stroke after COVID-19 infection. JAMA. 2022;328(9):887-889.
doi pubmed pmc - Gupta MD, Kunal S, M PG, Goyal D, Malhotra RK, Mishra P, Shukla M, et al. Impact of COVID-19 vaccination on mortality after acute myocardial infarction. PLoS One. 2023;18(9):e0291090.
doi pubmed pmc - Zahid B, Kamal M, Said M, Salem M, Elakabawi K. Effect of COVID-19 pandemic on six-month mortality and clinical outcomes of patients with ST-elevation myocardial infarction. Postepy Kardiol Interwencyjnej. 2022;18(3):228-236.
doi pubmed pmc - Jain V, Gupta K, Bhatia K, Bansal A, Arora S, Khandelwal AK, Rosenberg JR, et al. Management of STEMI during the COVID-19 pandemic: Lessons learned in 2020 to prepare for 2021. Trends Cardiovasc Med. 2021;31(3):135-140.
doi pubmed pmc - Bikdeli B, Madhavan MV, Jimenez D, Chuich T, Dreyfus I, Driggin E, Nigoghossian C, et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC State-of-the-Art review. J Am Coll Cardiol. 2020;75(23):2950-2973.
doi pubmed pmc - Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506.
doi pubmed pmc - Jiang J, Chan L, Kauffman J, Narula J, Charney AW, Oh W, Nadkarni G, et al. Impact of vaccination on major adverse cardiovascular events in patients with COVID-19 infection. J Am Coll Cardiol. 2023;81(9):928-930.
doi pubmed pmc - Jabagi MJ, Botton J, Bertrand M, Weill A, Farrington P, Zureik M, Dray-Spira R. Myocardial infarction, stroke, and pulmonary embolism after BNT162b2 mRNA COVID-19 vaccine in people aged 75 years or older. JAMA. 2022;327(1):80-82.
doi pubmed pmc - Lin DY, Gu Y, Xu Y, Wheeler B, Young H, Sunny SK, Moore Z, et al. Association of primary and booster vaccination and prior infection with SARS-CoV-2 infection and severe COVID-19 outcomes. JAMA. 2022;328(14):1415-1426.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.