

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 5, October 2024, pages 369-376

The Impact of Remote Ischemic Preconditioning on Inflammation Markers in Patients Undergoing Coronary Artery Bypass Grafting
Cezar Lucaa, b, Alexandra Boieriua, c, Daniela Neculoiua, d, Diana Tinta, e, f
aTransilvania University, Brasov, Romania
bCardiology Department, Cardiovascular Recovery Hospital, “Dr. Benedek Geza”, Covasna, Romania
cCardiology Department, Emergency Clinical County Hospital, Brasov, Romania
dClinical Laboratory Department, Emergency Clinical County Hospital, Brasov, Romania
eCardiology Department, Clinicco Hospital, Brasov, Romania
fCorresponding Author: Diana Tint, Faculty of Medicine, Transilvania University, Brasov 500036, Romania
Manuscript submitted July 15, 2024, accepted August 22, 2024, published online October 11, 2024
Short title: Ischemic Preconditioning and Inflammation Markers
doi: https://doi.org/10.14740/cr1702
| Abstract | ▴Top |
Background: This study aimed to investigate if remote ischemic preconditioning reduces the inflammatory process on patients undergoing coronary artery bypass grafting (CABG).
Methods: We conducted a case-control study involving 80 patients, half of whom underwent ischemic preconditioning for severe coronary artery disease (CAD) and subsequently underwent CABG. We assessed interleukin (IL)-1 and IL-6 levels using the enzyme-linked immunosorbent assay (ELISA) method, high-sensitivity troponin I (hsTnI) using chemiluminescent immunoassay (CLIA), and C-reactive protein (CRP) using the turbidimetric method at three key time points: before surgery (visit 1 or V1), immediately postoperatively (visit 2 or V2), and 1 week postoperatively (visit 3 or V3) in all subjects.
Results: Ischemic preconditioned patients showed a significant decrease in proinflammatory markers (IL-1, IL-6) but not in CRP or hsTnI.
Conclusions: This study demonstrated that remote ischemic preconditioning significantly reduced the levels of specific proinflammatory markers (IL-1 and IL-6), which may suggest general systemic protection. However, it did not demonstrate cardioprotection per se, as evidenced by the absence of a statistically significant decrease in hsTnI level.
Keywords: Remote ischemic preconditioning; Coronary artery bypass grafting; Interleukin-1; Interleukin-6; C-reactive protein; Inflammation
| Introduction | ▴Top |
Remote ischemic preconditioning (RIPC) stands as a noninvasive approach designed to protect the heart and other organs from the harmful effects of lethal ischemia and reperfusion injury. The method involves brief cycles of limb ischemia and reperfusion, typically carried out by alternately inflating and deflating a blood pressure cuff on one or more limbs to a suprasystolic pressure value for several cycles [1].
When organs are repeatedly exposed to short-term ischemia-reperfusion, less damage occurs during final reperfusion compared to prolonged ischemic episodes, for example, in patients undergoing coronary artery bypass grafting (CABG) and remote ischemic conditioning (RIC) [2, 3].
During CABG, there is a temporary interruption of blood supply to the heart and lungs, leading to the generation of oxygen free radicals. These elements prompt the upregulation of cell surface adhesion molecules and the expression of proinflammatory cytokines [4] such as interleukin (IL)-1 and IL-6. Furthermore, IL-6 appears as a potent inducer of C-reactive protein (CRP) synthesis in hepatocytes, as well as an activator of the coagulation cascade. Diffuse endothelial injury and microvascular thrombosis are possible effects between this interaction of inflammation and coagulation, leading also to increased serum troponin levels [5].
Przyklenk et al described the RIPC phenomena for the first time at the end of the 20th century [6]. After several years, the concept of “cardioprotection at a distance” through ischemia conditioning was soon expanded to other tissues and organs, as well as to greater distances from the heart [7]. The underlying mechanisms are likely to include transferable humoral release from perfused tissue, as well as neuronal responses [8].
RIPC was shown to improve clinical outcomes in patients undergoing surgical coronary revascularization under isoflurane anesthesia [9, 10]. However, several major phase III trials did not confirm the benefits of RIPC after cardiovascular surgery [10, 11].
This study aims to evaluate the impact of RIPC on inflammation markers in patients undergoing CABG. Future research should aim to clarify the specific clinical benefits of RIPC in CABG surgery. This could involve focusing on endpoints such as long-term survival, incidence of major adverse cardiac events (MACE), or quality of life improvements.
| Materials and Methods | ▴Top |
We conducted a prospective observational study in which we consecutively enrolled (Fig. 1) 80 adults patients (> 18 years) with severe coronary artery disease, undergoing elective CABG. These participants were then randomly assigned in a 1:1 ratio to either undergo RIPC or be part of the control group. All members responsible for conducting the study were blinded, and patients provided informed consent in order to participate. The exclusion criteria encompassed: the requirement for emergency CABG, history of prior revascularization, decompensated heart failure, left ventricular ejection fraction (LVEF) less than 30%, severe renal failure (grade 4 or under dialysis), hepatic dysfunction (Child 2), severe pulmonary disease, and the inability or refusal to provide informed consent.
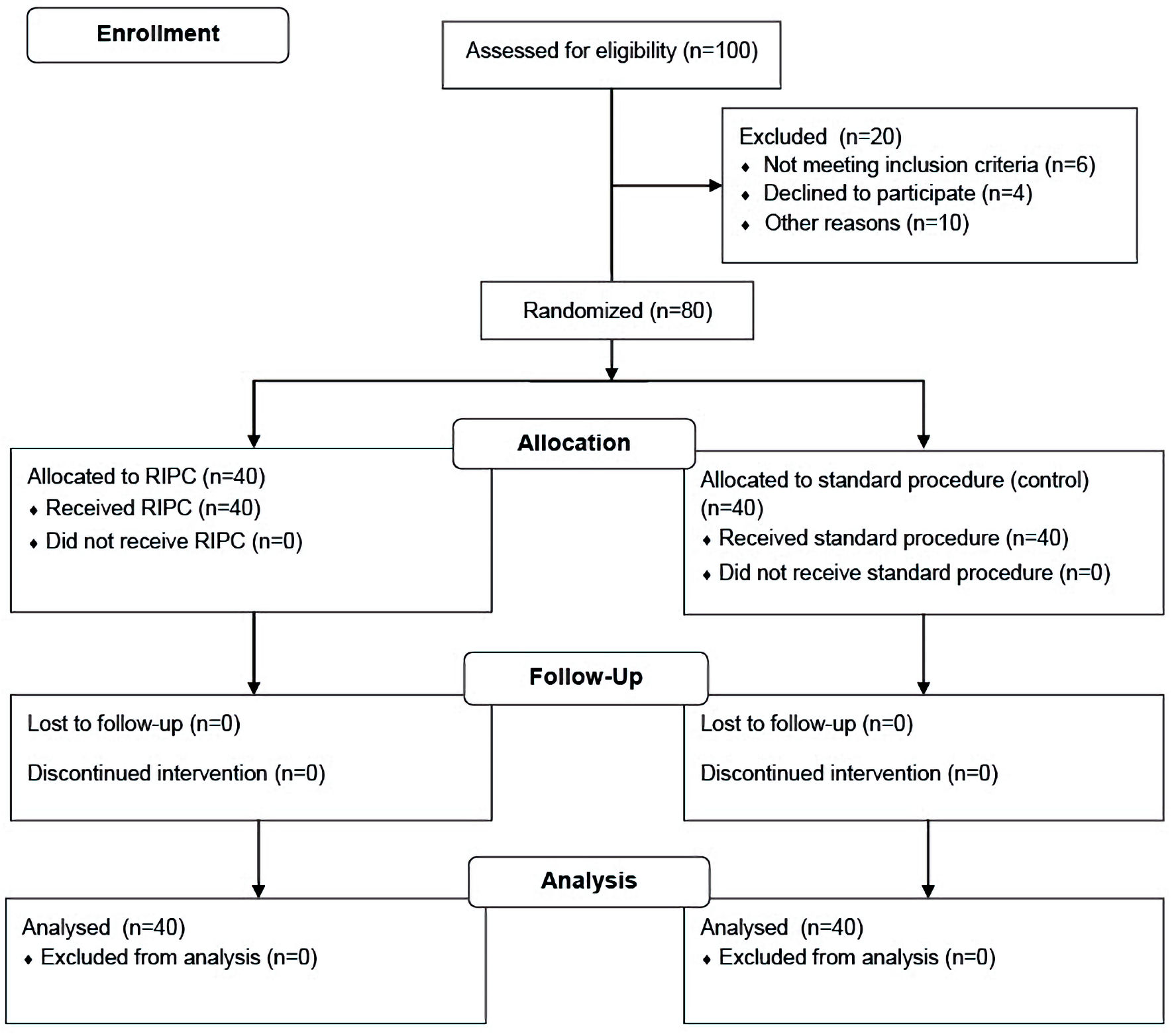 Click for large image | Figure 1. Randomization and follow-up flowchart. RIPC: remote ischemic preconditioning. |
The research was carried out at Clinicco Hospital in Brasov, spanning from January 2020 to November 2022. All procedures in this study were conducted in accordance with the Helsinki Declaration for research involving human subjects and obtained ethical approval from the Ethics Review Board of Transilvania University of Brasov.
Upon admission, patients underwent an initial evaluation comprising their past medical history and present clinical condition, alongside assessments from physical examinations, echocardiography, and laboratory tests. Venous blood samples were collected from each patient as part of the evaluation process.
Furthermore, we quantified the severity of coronary lesions using the Syntax score, which was based on the coronary angiography previously performed in all patients, approximately 2 to 4 weeks prior to the index hospitalization for CABG.
The procedure of RIPC was carried out on the day of surgery, before the induction of anesthesia. It consisted of inflating a blood pressure cuff on the upper and lower limbs to 200 mm Hg for 5 min (ischemia stage), followed by a 5-min time-out with the cuff deflated (reperfusion stage) for a total number of four cycles [1].
Anesthetic management, the cardio-pulmonary bypass, cardioplegia, surgical techniques and any other aspect of preoperative and postoperative management were in accordance with existing protocols in the hospital. All patients were subjected to the same types of general anesthetics (the volatile inhalation and intravenous hypnotic types).
Blood samples for blood cell counts, glycemia, renal function, hepatic function, cardiac biomarkers such as high-sensitivity troponin I (hsTnI), and other biological parameters were collected per hospital protocol.
For the specific parameters in our study, we processed the samples by centrifugation to separate the serum from the plasma, which were then labeled and stored at -80 °C. We assessed IL-1, IL-6 using the enzyme-linked immunosorbent assay (ELISA) test, hsTnI using chemiluminescent immunoassay (CLIA), and CRP using the turbidimetric method in both preconditioned and non-preconditioned populations at three key moments: before surgery (visit 1 or V1), immediately postoperatively (visit 2 or V2), and 1 week postoperatively (visit 3 or V3).
For IL-1 and IL-6, commercial ELISA kits are typically designed with highly specific antibodies that have minimal cross-reactivity with other cytokines. The specificity is often close to 100%, meaning that the antibodies used in the assay specifically bind to IL-1 or IL-6 without significant interference from other substances in the sample. Sensitivity is the ability of the ELISA to detect low concentrations of IL-1 or IL-6 in the sample.
Sensitivity for ELISA assays for IL-1 and IL-6 is usually in the range of pg/mL. For example, a typical sensitivity might be around 0.1 to 10 pg/mL for both IL-1 and IL-6, as indicated in the instructions for the kit we used.
The specificity and sensitivity for CLIA and turbidimetric methods for determining high-sensitive troponin and CRP levels are reported to be very high (> 90%) in the information provided by the kits used by us, allowing for the detection of these markers in a significant majority of individuals even at low levels.
The database has been created using Microsoft Excel 2019, and values have been interpreted by IBM Spss 26.0. Categorical variables were given as counts or absolute frequencies. To observe the difference between the mean values of two variables, we used Student’s t-test or Mann-Whitney U (normal distribution or not), and values of P < 0.05 were considered statistically significant. Post hoc analyses, in analysis of variance with repeated measures (ANOVA RM), determined the differences within and between groups.
The parameters for the power analysis included an expected effect size of Cohen’s d = 0.5 for a medium effect, a significance level (alpha) of 0.05, and a target power of 0.80. This power level was chosen to provide an 80% probability of detecting a true effect, if it exists, thereby balancing the risk of type I (false positive) and type II (false negative) errors.
| Results | ▴Top |
A summary of the baseline, clinical and operative characteristics of all participants is provided in Table 1.
 Click to view | Table 1. Baseline, Clinical and Operative Characteristics of the Patients |
There were no significant differences between the groups in terms of age, gender distribution, cardiovascular risk factors, or comorbidities. The severity of coronary artery disease, assessed using the Syntax score, was also found to be comparable across both groups. Furthermore, there were no significant variations between the groups in terms of aortic clamping time, cardio-pulmonary bypass time, the duration of time spent in the intensive care unit (ICU) and overall hospitalization duration.
RIPC led to a significant reduction of the total value of inflammatory markers (IL-1, IL-6). Consequently, within the preconditioned group, the IL-1 levels decreased at visits 2 and 3 in contrast to the non-preconditioned group, where IL-1 levels exhibited an increase (V2 (pg/mL): 2.85 ± 2.24 vs. 5.56 ± 4.90, P = 0.0021; V3 (pg/mL): 2.75 ± 2.06 vs. 6.54 ± 5.10, P < 0.0001). IL-6 also exhibited a significant decrease in preconditioned patients compared to non-preconditioned patients, wherein the reduction in the level of this marker was notably pronounced (V2 (pg/mL): 16.43 ± 9.73 vs. 22.83 ± 13.39, P = 0.01; V3 (pg/mL): 2.75 ± 2.06 vs. 6.54 ± 5.10, P < 0.0001).
Significant reductions in the total levels of inflammatory markers (IL-1, IL-6) were observed with RIPC. Consequently, compared to the non-preconditioned group, where IL-1 levels displayed an upward trend (V2 (pg/mL): 2.85 ± 2.24 vs. 5.56 ± 4.90, P = 0.0021; V3 (pg/mL): 2.75 ± 2.06 vs. 6.54 ± 5.10, P < 0.0001), the IL-1 levels in the preconditioned group decreased at visits 2 and 3. IL-6 also showed a significant decrease, when comparing preconditioned to non-preconditioned subjects (V2 (pg/mL): 16.43 ± 9.73 vs. 22.83 ± 13.39, P = 0.01); V3 (pg/mL): 2.75 ± 2.06 vs. 6.54 ± 5.10, P < 0.0001).
The statistically significant changes observed in the plasma levels of both variables indicate that RIPC leads to a decrease in inflammatory markers among patients undergoing CABG.
In our study hsTnI and CRP were also assessed, and it is noteworthy that the decrease in their plasma levels in the preconditioned group did not reach statistical significance (hsTnI V2 (pg/mL): 0.97 ± 0.76 vs. 1.22 ± 0.97, P = 0.20; V3 (pg/mL): 0.91 ± 0.69 vs. 1.04 ± 0.80, P = 0.43; CRP V2 (mg/dL): 6.35 ± 4.28 vs. 6.43 ± 4.36, P = 0.93; V3 (mg/dL): 2.18 ± 1.38 vs. 2.31 ± 1.54, P = 0.69), as depicted in Table 2.
Click to view | Table 2. IL-1, IL-6, hsTnI and CRP Under RIPC on Patients Undergoing CABG |
| Discussion | ▴Top |
The process known as RIPC describes how short episodes of non-fatal ischemia in one organ or tissue might make a different organ or tissue resistant to prolonged ischemic shocks in later stages. This process can be used in all patients with ischemic heart disease and in those who are undergoing CABG surgery [1].
This method was first described by Murry et al in 1986 in a study on the heart of dogs [12], which demonstrated the adaptability of the heart to ischemic episodes lasting several minutes, a phenomenon termed ischemic preconditioning (IP) [13, 14].
Kuntscher et al demonstrated in a laboratory mouse study that acute RIPC in the cremaster muscle has a protective effect due to increased capillary perfusion and decreased postcapillary inflammatory response [15]. It has also been observed that brief episodes of arterial occlusion such as renal, mesenteric or muscular artery occlusion provide cardiac protection through humoral and/or neurological mechanisms [3].
In recent years, studies have also been carried out on humans, by tightening the upper or lower limbs with a tourniquet, the technique being easy to implement and bringing successful results [16]. It has also been shown that the protective effect of RIPC on myocardial tissue can be induced with blood transfusions from a donor organism undergoing preconditioning [17]. Transferring the protective effect distally, to organs via blood circulation, led to the idea that this effect can also be transferred between individuals. Later, Orhan et al showed that IP had a protective effect, transferable between individuals with the help of blood serum [18].
Moreover, our study’s results did not demonstrate statistically significant decreases in hsTnI and CRP, in contrast to other studies that demonstrated cardiac protection by statistically significant reductions in hsTnT values and inflammatory markers (IL-6, IL-8, IL-10, tumor necrosis factor alpha (TNF-α)) [19-21].
RIPC produces an immediate improvement in the coronary flow reserve and the index of microcirculatory resistance [22]. This suggests that RIPC may improve coronary microcirculatory performance, which in turn provides cardioprotection following percutaneous coronary intervention [23].
In contrast, several publications (Moscarelli et al 2019 [24], Pinaud et al 2016 [25], and Hausenloy et al 2019 [16]) found that RIC applied to an upper limb prior to CABG, aortic valve replacement [24, 25] or primary percutaneous angioplasty failed to reduce infarct size, as evidenced by elevated hsTnT, troponin I and the absence of decreased inflammatory markers (IL-6, IL-8, IL-10 and TNF-α values) [10]. These findings differ from the results of a previous paper by the same authors in which RIPC applied to an upper limb before primary percutaneous angioplasty reduced infarct size as evidenced by single photon emission computed tomography (SPECT) [26].
In the majority of published papers, the RIPC protocol typically involves the utilization of a single limb, primarily the upper limb, undergoing three cycles of 5 min of ischemia followed by reperfusion [27-30]. Other studies used only one of the lower limbs [31, 32], while others inflated a blood pressure cuff to 200 mm Hg in both the upper and lower limbs at the same time [33], in contrast with our study protocol that included the use of each limb with a 5-min ischemia-reperfusion cycle.
In our study, unlike those previously mentioned, cardiac protection was noted through a reduction in IL-1 and IL-6 levels, although there was not a statistically significant decrease observed in CRP and hsTnI values. It is worth noting that literature cites significant troponin reduction in preconditioned patients compared to those who did not undergo RIPC [34, 35].
As previously mentioned, although IL-6 is recognized as a potent inducer of CRP synthesis in hepatocytes, we were unable to establish a statistically significant correlation in this regard.
It is worth noting that, compared to our paper, other studies have demonstrated cardioprotection in ischemic preconditioned patients by significantly reducing CRP and plasminogen activator inhibitor-1 (PAI-1) values [36], increasing flow-mediated dilation, and significantly decreasing the levels of hsTnI [34], decreasing the total values of CRP and calprotectin (inflammation markers) [37], or increasing flow-mediated dilation by 40% [38].
The variability in outcomes could be attributed to several factors, including differences in study design, patient populations, timing and protocols of RIPC application, and the specific endpoints measured. 1) Study design and methodology: Different studies might employ varying protocols for RIPC, such as the number of cycles, duration, and timing relative to the intervention or insult (e.g., surgery). These methodological differences could lead to inconsistent results. 2) Patient population: The characteristics of the patient populations studied, including age, comorbidities, and baseline risk factors, can significantly influence the outcomes of RIPC. Studies involving more heterogeneous populations may report more variable effects. 3) Endpoints and outcome measures: The definition of endpoints, whether clinical (e.g., mortality, major adverse cardiovascular events) or biomarker-based (e.g., levels of troponin, high-sensitivity CRP (hsCRP)), could result in different conclusions about the efficacy of RIPC. 4) Timing of RIPC application: The timing of RIPC in relation to the ischemic event or surgical procedure is critical. Variations in the timing across studies may account for differences in observed efficacy. 5) Sample size and statistical power: Studies with small sample sizes may be underpowered to detect significant differences, leading to variability in reported results. Conversely, larger studies might show more consistent effects due to greater statistical power.
Given these factors, the disparity in results should not necessarily be interpreted as a lack of efficacy of RIPC but rather as a reflection of the complexities involved in studying this intervention. Future research should aim to standardize protocols and identify the specific patient populations and conditions under which RIPC is most effective. By addressing these issues, the field can move towards more consistent and generalizable findings.
In reviewing the literature, it was observed that various publications have utilized relatively small sample sizes, which can significantly impact the consistency and reliability of research findings. Small sample sizes can lead to increased variability, reduced statistical power, effect size inflation and lack of generalizability. The disparity in results observed across various publications may, therefore, be partially attributed to differences in sample sizes and the corresponding power of these studies. Studies with larger sample sizes tend to produce more reliable and consistent results, as they are better equipped to detect true effects and minimize the influence of random variability.
The suitability of applying RIPC for only 1 day is a topic of ongoing debate and research. The effectiveness of a single-day application largely depends on the specific clinical context, the timing relative to the ischemic event, and the intended outcomes. In some acute clinical settings, such as prior to surgery or a planned ischemic event, a single day of RIPC might be sufficient to confer protective effects. Studies have shown that RIPC can reduce myocardial injury during cardiac surgery when applied immediately before the procedure [39]. The timing of RIPC is critical. Preconditioning shortly before the ischemic event may trigger protective mechanisms, such as the release of protective cytokines, activation of cellular pathways, and increased tissue tolerance to ischemia. If the RIPC is applied too far in advance, its effects might diminish by the time the ischemic event occurs [40]. While RIPC applied for 1 day may be adequate in certain acute clinical scenarios, its efficacy might be limited depending on the timing, the nature of the ischemic event, and the specific clinical outcomes being targeted. Further research is needed to determine the optimal duration and frequency of RIPC application for different clinical situations.
The methodologies used for measuring IL-1, IL-6, CRP, and high-sensitivity troponin (hsTn) share common principles, such as immunodetection, but there are significant differences in sensitivity, specificity, and practicality that can impact the results of RIPC studies. ELISA remains the gold standard for cytokine and CRP measurement, but the introduction of high-sensitivity assays (CLIA), such as those for hsTn, has enhanced the ability to detect minute changes in biomarker levels. The choice of methodology can influence the interpretation of results, and thus, it is crucial for studies to standardize methods or account for methodological differences when comparing findings [9, 41, 42].
The significant reduction observed in our study regarding the inflammatory markers like IL-1 and IL-6 suggests that RIPC may have some anti-inflammatory effects, which is a positive outcome. However, the lack of impact on key biomarkers such as hsTnI, raises questions about the overall direct cardioprotection efficacy of RIPC in this context. Even if we do not observe an improvement in short-term cardiac events, it is also important to consider the long-term effects of RIPC on cardiac function and survival rates post-surgery. Although immediate biomarker responses are important, the ultimate goal is to improve long-term patient outcomes, including reducing the risk of future cardiac events.
One limitation of this study is the relatively small sample size, which may have limited the statistical power to detect smaller effects, increasing the risk of type II errors and potentially affecting the generalizability of the findings (Tables 3, 4).
Click to view | Table 3. Post-Hoc Power Analysis |
Click to view | Table 4. Power by Effect Size |
Conclusions
This study demonstrates that RIPC significantly reduced the levels of specific proinflammatory markers (IL-1 and IL-6), which may suggest general systemic protection. However, it did not demonstrate cardioprotection per se, as evidenced by the absence of a statistically significant decrease in hsTnI level.
Acknowledgments
We are grateful for the support provided by the Transilvania University of Brasov.
Financial Disclosure
There was no specific funding source to be mentioned.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Written informed consent was obtained from all subjects.
Author Contributions
CL and DT designed the study. CL conducted the research and drafted the manuscript, while DT performed critical editing. AB and DN assisted with sample collection and statistical analysis. DT carefully supervised the manuscript preparation and writing.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
CABG: coronary artery bypass grafting; CAD: coronary artery disease; CBP: cardio-pulmonary bypass; CLIA: chemiluminescent immunoassay; RIC: remote ischemic conditioning; hsTnI: high-sensitivity troponin I; ICU: intensive care unit; IL: interleukin-1; LVEF: left ventricular ejection fraction; CRP: C-reactive protein; IP: ischemic preconditioning; RIPC: remote ischemic preconditioning; TNF-α: tumor necrosis factor alpha
| References | ▴Top |
- Lang JA, Kim J. Remote ischaemic preconditioning - translating cardiovascular benefits to humans. J Physiol. 2022;600(13):3053-3067.
doi pubmed pmc - Laurikka J, Wu ZK, Iisalo P, Kaukinen L, Honkonen EL, Kaukinen S, Tarkka MR. Regional ischemic preconditioning enhances myocardial performance in off-pump coronary artery bypass grafting. Chest. 2002;121(4):1183-1189.
doi pubmed - Gunata M, Parlakpinar H. A review of myocardial ischaemia/reperfusion injury: Pathophysiology, experimental models, biomarkers, genetics and pharmacological treatment. Cell Biochem Funct. 2021;39(2):190-217.
doi pubmed - Kolaczkowska E, Kubes P. Neutrophil recruitment and function in health and inflammation. Nat Rev Immunol. 2013;13(3):159-175.
doi pubmed - Su JH, Luo MY, Liang N, Gong SX, Chen W, Huang WQ, Tian Y, et al. Interleukin-6: a novel target for cardio-cerebrovascular diseases. Front Pharmacol. 2021;12:745061.
doi pubmed pmc - Przyklenk K, Bauer B, Ovize M, Kloner RA, Whittaker P. Regional ischemic 'preconditioning' protects remote virgin myocardium from subsequent sustained coronary occlusion. Circulation. 1993;87(3):893-899.
doi pubmed - Heusch G. 25 years of remote ischemic conditioning: from laboratory curiosity to clinical outcome. Basic Res Cardiol. 2018;113(3):15.
doi pubmed - Heusch G, Botker HE, Przyklenk K, Redington A, Yellon D. Remote ischemic conditioning. J Am Coll Cardiol. 2015;65(2):177-195.
doi pubmed pmc - Thielmann M, Kottenberg E, Kleinbongard P, Wendt D, Gedik N, Pasa S, Price V, et al. Cardioprotective and prognostic effects of remote ischaemic preconditioning in patients undergoing coronary artery bypass surgery: a single-centre randomised, double-blind, controlled trial. Lancet. 2013;382(9892):597-604.
doi pubmed - Kleinbongard P, Peters J, Jakob H, Heusch G, Thielmann M. Persistent survival benefit from remote ischemic pre-conditioning in patients undergoing coronary artery bypass surgery. J Am Coll Cardiol. 2018;71(2):252-254.
doi pubmed - Hausenloy DJ, Candilio L, Evans R, Ariti C, Jenkins DP, Kolvekar S, Knight R, et al. Remote ischemic preconditioning and outcomes of cardiac surgery. N Engl J Med. 2015;373(15):1408-1417.
doi pubmed - Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74(5):1124-1136.
doi pubmed - Liu GS, Stanley AW, Downey JM. Ischaemic preconditioning is not dependent on neutrophils or glycolytic substrate at reperfusion in rabbit heart. Cardiovasc Res. 1992;26(12):1195-1198.
doi pubmed - Vahlhaus C, Schulz R, Post H, Rose J, Heusch G. Prevention of ischemic preconditioning only by combined inhibition of protein kinase C and protein tyrosine kinase in pigs. J Mol Cell Cardiol. 1998;30(2):197-209.
doi pubmed - Kuntscher MV, Kastell T, Sauerbier M, Nobiling R, Gebhard MM, Germann G. Acute remote ischemic preconditioning on a rat cremasteric muscle flap model. Microsurgery. 2002;22(6):221-226.
doi pubmed - Hausenloy DJ, Kharbanda RK, Moller UK, Ramlall M, Aaroe J, Butler R, Bulluck H, et al. Effect of remote ischaemic conditioning on clinical outcomes in patients with acute myocardial infarction (CONDI-2/ERIC-PPCI): a single-blind randomised controlled trial. Lancet. 2019;394(10207):1415-1424.
doi pubmed pmc - Dickson EW, Reinhardt CP, Renzi FP, Becker RC, Porcaro WA, Heard SO. Ischemic preconditioning may be transferable via whole blood transfusion: preliminary evidence. J Thromb Thrombolysis. 1999;8(2):123-129.
doi pubmed - Orhan E, Gunduz O, Kaya O, Oznur M, Sahin E. Transferring the protective effect of remote ischemic preconditioning on skin flap among rats by blood serum. J Plast Surg Hand Surg. 2019;53(4):198-203.
doi pubmed - Wang H, Lyu Y, Liao Q, Jin L, Xu L, Hu Y, Yu Y, et al. Effects of remote ischemic preconditioning in patients undergoing off-pump coronary artery bypass graft surgery. Front Physiol. 2019;10:495.
doi pubmed pmc - Gorjipour F, Saeedzadeh T, Toloueitabar Y, Kachoueian N, Bahlouli Ghashghaei S, Mortazian M, Dehghani Firoozabadi M, et al. Remote ischemic preconditioning effects on inflammatory markers and myocardial protection in coronary artery bypass graft surgery. Perfusion. 2022;37(1):56-61.
doi pubmed - Jin X, Wang L, Li L, Zhao X. Protective effect of remote ischemic pre-conditioning on patients undergoing cardiac bypass valve replacement surgery: A randomized controlled trial. Exp Ther Med. 2019;17(3):2099-2106.
doi pubmed pmc - Lau JK, Roy P, Javadzadegan A, Moshfegh A, Fearon WF, Ng M, Lowe H, et al. Remote Ischemic Preconditioning Acutely Improves Coronary Microcirculatory Function. J Am Heart Assoc. 2018;7(19):e009058.
doi pubmed pmc - Zhao ZZ, Li E, Li XJ, Guo Q, Shi QB, Li MW. Effects of remote ischemic preconditioning on coronary blood flow and microcirculation. BMC Cardiovasc Disord. 2023;23(1):404.
doi pubmed pmc - Moscarelli M, Fiorentino F, Suleiman MS, Emanueli C, Reeves BC, Punjabi PP, Angelini GD. Remote ischaemic preconditioning in isolated aortic valve and coronary artery bypass surgery: a randomized trialdagger. Eur J Cardiothorac Surg. 2019;55(5):905-912.
doi pubmed pmc - Pinaud F, Corbeau JJ, Baufreton C, Binuani JP, De Brux JL, Fouquet O, Angoulvant D, et al. Remote ischemic preconditioning in aortic valve surgery: Results of a randomized controlled study. J Cardiol. 2016;67(1):36-41.
doi pubmed - Botker HE, Kharbanda R, Schmidt MR, Bottcher M, Kaltoft AK, Terkelsen CJ, Munk K, et al. Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial. Lancet. 2010;375(9716):727-734.
doi pubmed - Venugopal V, Hausenloy DJ, Ludman A, Di Salvo C, Kolvekar S, Yap J, Lawrence D, et al. Remote ischaemic preconditioning reduces myocardial injury in patients undergoing cardiac surgery with cold-blood cardioplegia: a randomised controlled trial. Heart. 2009;95(19):1567-1571.
doi pubmed - Hausenloy DJ, Mwamure PK, Venugopal V, Harris J, Barnard M, Grundy E, Ashley E, et al. Effect of remote ischaemic preconditioning on myocardial injury in patients undergoing coronary artery bypass graft surgery: a randomised controlled trial. Lancet. 2007;370(9587):575-579.
doi pubmed - Kottenberg E, Thielmann M, Bergmann L, Heine T, Jakob H, Heusch G, Peters J. Protection by remote ischemic preconditioning during coronary artery bypass graft surgery with isoflurane but not propofol - a clinical trial. Acta Anaesthesiol Scand. 2012;56(1):30-38.
doi pubmed - Wagner R, Piler P, Bedanova H, Adamek P, Grodecka L, Freiberger T. Myocardial injury is decreased by late remote ischaemic preconditioning and aggravated by tramadol in patients undergoing cardiac surgery: a randomised controlled trial. Interact Cardiovasc Thorac Surg. 2010;11(6):758-762.
doi pubmed - Cheung MM, Kharbanda RK, Konstantinov IE, Shimizu M, Frndova H, Li J, Holtby HM, et al. Randomized controlled trial of the effects of remote ischemic preconditioning on children undergoing cardiac surgery: first clinical application in humans. J Am Coll Cardiol. 2006;47(11):2277-2282.
doi pubmed - Candilio L, Malik A, Ariti C, Barnard M, Di Salvo C, Lawrence D, Hayward M, et al. Effect of remote ischaemic preconditioning on clinical outcomes in patients undergoing cardiac bypass surgery: a randomised controlled clinical trial. Heart. 2015;101(3):185-192.
doi pubmed - Nichols M, Townsend N, Scarborough P, Rayner M. Cardiovascular disease in Europe 2014: epidemiological update. Eur Heart J. 2014;35(42):2950-2959.
doi pubmed - Liang Y, Li YP, He F, Liu XQ, Zhang JY. Long-term, regular remote ischemic preconditioning improves endothelial function in patients with coronary heart disease. Braz J Med Biol Res. 2015;48(6):568-576.
doi pubmed pmc - Zhou C, Liu Y, Yao Y, Zhou S, Fang N, Wang W, Li L. beta-blockers and volatile anesthetics may attenuate cardioprotection by remote preconditioning in adult cardiac surgery: a meta-analysis of 15 randomized trials. J Cardiothorac Vasc Anesth. 2013;27(2):305-311.
doi pubmed - Meng R, Ding Y, Asmaro K, Brogan D, Meng L, Sui M, Shi J, et al. Ischemic Conditioning Is Safe and Effective for Octo- and Nonagenarians in Stroke Prevention and Treatment. Neurotherapeutics. 2015;12(3):667-677.
doi pubmed pmc - Pryds K, Rahbek Schmidt M, Bjerre M, Thiel S, Refsgaard J, Botker HE, Drage Ostgard R, et al. Effect of long-term remote ischemic conditioning on inflammation and cardiac remodeling. Scand Cardiovasc J. 2019;53(4):183-191.
doi pubmed - Hyngstrom AS, Nguyen JN, Wright MT, Tarima SS, Schmit BD, Gutterman DD, Durand MJ. Two weeks of remote ischemic conditioning improves brachial artery flow mediated dilation in chronic stroke survivors. J Appl Physiol (1985). 2020;129(6):1348-1354.
doi pubmed pmc - Meybohm P, Bein B, Brosteanu O, Cremer J, Gruenewald M, Stoppe C, Coburn M, et al. A Multicenter Trial of Remote Ischemic Preconditioning for Heart Surgery. N Engl J Med. 2015;373(15):1397-1407.
doi pubmed - Yildirim F, Iskesen I, Kurdal AT, Ozturk T, Taneli F, Gozukara C, Ozbakkaloglu A. Is "Attenuation of Oxidative Stress" Helpful to Understand the Mechanism of Remote Ischemic Preconditioning in Cardiac Surgery? J Cardiothorac Vasc Anesth. 2016;30(1):134-140.
doi pubmed - Heusch G. Molecular basis of cardioprotection: signal transduction in ischemic pre-, post-, and remote conditioning. Circ Res. 2015;116(4):674-699.
doi pubmed - Altman R, Shankaran S. Remote ischemic preconditioning: mechanisms and applications. Indian Journal of Thoracic and Cardiovascular Surgery. 2020;36:16-26.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.