

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Original Article
Volume 8, Number 5, October 2017, pages 199-205
In-Hospital Clinical Outcomes and Procedural Complications of Percutaneous Coronary Intervention in Elderly Patients
Seyed Fakhreddin Hejazia, Leili Iranirada, Kobra Doostalia, c, Narges Khodadadib, Sameeye Norouzia
aDepartment of Cardiology, Shahid Beheshti, Qom University of Medical Science and Health Services, Qom, Iran
bDepartment of Medicine, Shahid Beheshti, Qom University of Medical Science and Health Services, Qom, Iran
cCorresponding Author: Kobra Doostali, Department of Cardiology, Shahid Beheshti, Qom University of Medical Science and Health Services, Qom, Iran
Manuscript submitted July 5, 2017, accepted August 8, 2017
Short title: PCI in Elderly Patients
doi: https://doi.org/10.14740/cr582e
| Abstract | ▴Top |
Background: As population growth leads to an increase in the number of the elderly with coronary artery disease, an evaluation of the clinical outcomes of percutaneous coronary intervention (PCI) in the elderly patients seems to be essential.
Methods: A prospective, observational cohort study was performed on 468 patients in two groups of elderly and non-elderly patients (mean age: 60.01 ± 10.84 years; ≥ 70 years, 20.1%; men, 62%) who underwent PCI, to evaluate the procedural success and in-hospital major and minor adverse cardiovascular events in the elderly patients.
Results: The procedural success rate was significantly lower (95.7% vs. 99.5%, P = 0.017) and the rates of in-hospital complications were significantly higher (10.6% vs. 0.8%, P < 0.0001) in elderly (+70) than in non-elderly patients. On the basis of a multivariate analysis, being elderly was not an independent predictor of procedural failure, but increased the chance of in-hospital complications to 8% higher (odds ratio: 0.08; 95% confidence interval: 0.01 - 0.39; P = 0.002).
Conclusion: Regardless of the difference in the procedural success and in-hospital complication rates between our two study groups, aging is not an important predictor of them. Furthermore, PCI should not be refused in elderly patients if indicated.
Keywords: Elderly; Major adverse cardiovascular events; Percutaneous coronary intervention
| Introduction | ▴Top |
The growth of the country’s population age reflects the stage of the transition of the population structure from youth to aging. According to the results of 2011 census, assuming the stability of current trends of birth, aging of the population in 2041 reaches about 20%. Accordingly, it is estimated that the beginning of the 15th century is the beginning of the growing elderly population in Iran [1, 2]. The increasing growth rate of elderly population compared to the country’s population growth and the projected increase in the number and proportion of elderly in the coming years emphasizes the need for attention and care of more health and treatment in this age group with the aim of achieving more effective clinical and therapeutic approaches.
Increasing age is associated with increased incidence of atherosclerosis and cardiovascular diseases (CVDs), including ischemic heart disease (IHD) and coronary artery disease (CAD). Today, more than any other disease in the developed world, IHD causes death and disability, and disability imposes a high economic cost. Epicardial coronary artery atherosclerosis is the most common cause of myocardial ischemia. Age, left ventricular (LV) function, position and severity of coronary artery stenosis and severity of myocardial ischemia are key indicators of prognosis in patients with IHD.
In general, if the number and severity of risk factors for atherosclerosis, such as hypertension, dyslipidemia, diabetes, morbid obesity, and history of myocardial infarction (MI) are more, the prognosis of patients with angina pectoris will be poor [3]. As a result, aging is an independent risk factor for atherosclerosis and prediction of cardiovascular events [4-6]. So, change of the age structure of the population will lead to a significant increase in the number of elderly patients with CVD, who underwent coronary revascularization [7]. Coronary revascularization consists of two main techniques: coronary artery bypass surgery (CABG) and percutaneous coronary intervention (PCI). More than half of patients with symptomatic IHD that needed revascularization can be treated with PCI. PCI is the most common method of revascularization in America and often is done twice as CABG. Balloon angioplasty and coronary stenting are the basis of PCI. Successful PCI compared to CABG is less costly and less invasive, requires a shorter hospital stay and provides patient earlier for resuming his active life. At the same time, the possibility of the repetition of angiography and the need for revascularization in PCI group are more than in CABG group. For this reason, its economic advantage is reduced over time because of more need to follow-up and probably a repeat of the actions [3]. Recently, several trials showed the effectiveness of PCI versus medical therapy in patients with symptomatic CAD. Significant improvement in symptoms, increased quality of life and reduced major adverse cardiovascular events in 1-year trials on comparing these two treatment approaches have been in favor of PCI. In the elderly population, revascularization with PCI method is more efficient and effective than medical therapy to relieve symptoms and quality of life. However, after a year of starting both treatments, the primary differences raised in favor of PCI are dimmed [7-10]. Elderly patients are more likely to have significant comorbidities and more complex and chronic coronary lesions [11]. Therefore, aging can be stated as a factor for the occurrence of a lower rate of the success of PCI. This faces both the patient and physician with uncertainty to perform PCI as the optimal treatment for the elderly. So far, the clinical outcomes of PCI in elderly patients are not clear, so evaluation of clinical implications of this therapeutic approach for elderly patients in our country is essential. Accordingly, the purpose of this trial is to evaluate the practical success of PCI and the incidence of complications during the hospital stay in the elderly patients.
| Materials and Methods | ▴Top |
Study population
This was a prospective cohort study. Patients over 70 years old or lower with CAD ((acute coronary syndrome/stable angina) and candidates for PCI (n = 486) referred to the Shahid Beheshti Hospital of Qom, in October 2014 to August 2015 were assigned into two groups.
Study method
In this prospective study, patients referred to Shahid Beheshti Hospital of Qom during October 2014 to September 2015, after clinical and diagnostic assessment, candidates for angioplasty in the center according to the inclusion criteria, were studied. At first, the demographic data of patients, including age, gender, underlying diseases (diabetes, hypertension, dyslipidemia, and heart failure (HF)), clinical records (atrial fibrillation (AF), CABG, PCI, intracerebral hemorrhage (ICH), MI, cerebrovascular accident (CVA) and smoking) and therapeutic measures were recorded in a designed checklist. Moreover, based on the results of echocardiography and angiography, the left ventricular ejection fraction (LVEF) level and type of coronary artery of the patients were identified and inserted into the checklist. The anatomical success was defined as the attainment of a residual diameter stenosis of 20% and normal epicardial flow (TIMI-3 flow) and practical success was considered an anatomical success without major complication and relevant complications during hospitalization were examined.
Data collection
Data were collected with reference to the information recorded in patients undergoing PCI.
Data collection tools
A checklist and angiography report was used for collecting data.
Data analysis
All data collected were analyzed by SPSS 22. For qualitative variables, relative and absolute frequencies were calculated, and for quantitative variables, the mean and standard deviation were calculated. To determine the relationship between variables, Chi-square test or Fisher’s exact test and Phi and Cramer’s V and Pearson/Spearman correlation coefficients, with a significance level less than 0.05 were used. To determine the effect of independent variables on the dependent variables of the study, the multivariate logistic regression test was used.
| Results | ▴Top |
Demographic and clinical characteristics of patients in the two groups separately are shown in Table 1. Of 486 patients in the study, 20.1% were aged above 70 years with a mean age of 76.28 ± 4.59 years. Of the patients, 62% were men and sex composition of the two age groups was significantly different, so that the ratio of men to women in the age group below 70 years was higher (64.4% vs. 52.1%; P = 0.028).
 Click to view | Table 1. Demographic and Clinical Characteristics of Patients Separately in the Two Age Groups |
Rates of comorbidities such as diabetes, blood pressure, dyslipidemia and the history of ICH, CVA and MI in the two groups were not significantly different, although the prevalence of diabetes and dyslipidemia and the history of the CVA in younger patients was higher. At the same time, the prevalence of chronic renal failure and HF in the elderly was significantly higher (chronic kidney injury (CKI): P = 0.0001; HF: P = 0.011). Furthermore, LV dysfunction in the elderly was more than in younger patients (31.9% vs. 20.1%; P = 0.014) (Table 1).
In this study, 98.5% of patients using DES and only seven cases with BMS were under PCI. The PCI procedure in the two groups was not significantly different (P = 0.148) (Table 2).
Click to view | Table 2. Manifestations of the Coronary Artery Disease and Method for Performing PCI |
There was a significant relationship between elderly (over 70 years) and synchronous coronary multi-vessel stenosis (Cramer’s V = 0.121, P = 0.032 and 44.8% vs. 32.9%) (Fig. 1). According to Cramer’s V coefficient, the intensity of the relationship is weak. Percentage of elderly patients with multi-vessel coronary disease is more than patients under 70 years that shows the more prevalence of synchronous coronary multi-vessel stenosis in the elderly.
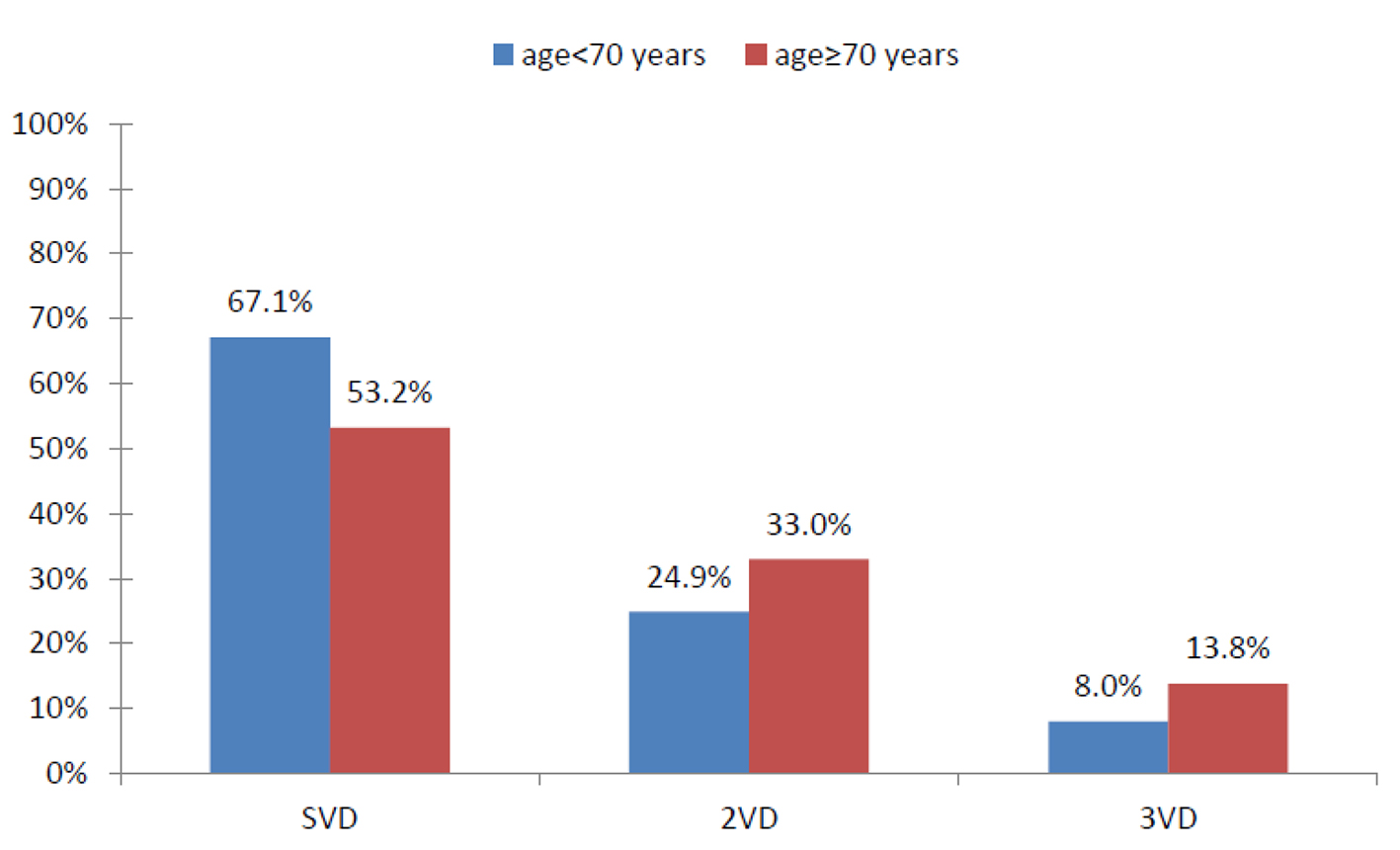 Click for large image | Figure 1. Ratio of the frequency of coronary artery atherosclerosis in two age groups. |
The manifestation of CAD in 60.3% and 39.7% of patients was in the form of ACS and stable angina, respectively. Although the percentage of manifestation of ACS in the elderly was higher, no significant difference was observed between the two age groups as well as no significant relationship between aging and the manifestation of CAD (68.1% vs. 58.3%, Cramer’s V = 0.87, P = 0.316) (Fig. 2).
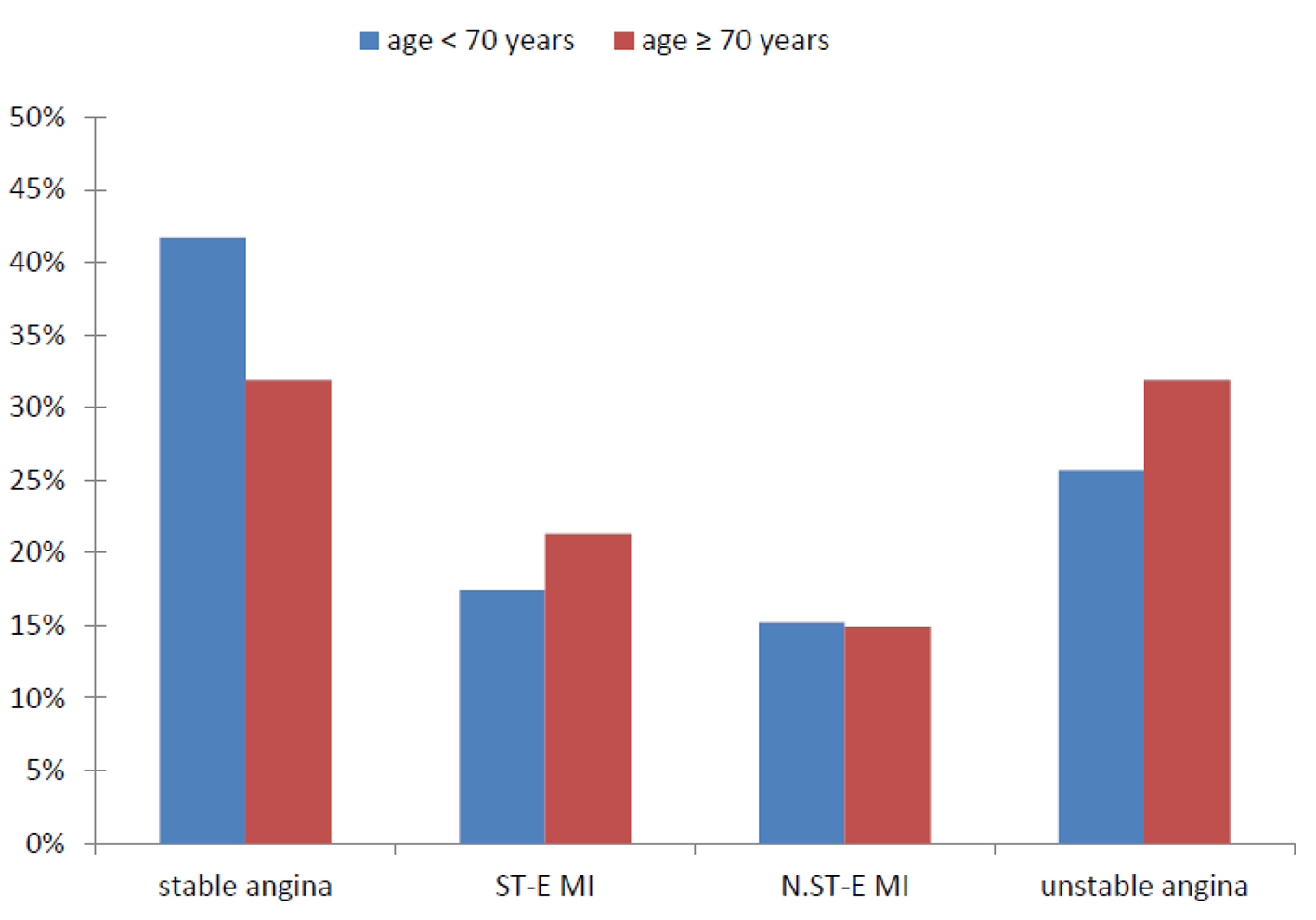 Click for large image | Figure 2. Frequency of different manifestations of CAD in two age groups of the patients. |
The percentage of occurrence of any of the side effects separately in two age groups is expressed in Table 3. Overall, 2.8% of patients have complicated that more percentage of the patients were elderly (three patients below 70 years versus 10 of the elderly population (P = 0.0001).
Click to view | Table 3. Complications After PCI During Hospitalization |
The practical success of PCI was obtained in 98.6% of patients. Due to a higher incidence of major adverse cardiovascular complications in elderly patients during hospitalization, the practical success of PCI significantly in the target age group (over 70 years) was lower (99.5% vs. 95.7%, Phi-Cramer = 0.132; P < 0.017).
Based on the results of the multivariate logistic correlation test, only one factor has been known in the success of PCI effective action. In this study due to the countable number of practical failures of PCI, AF is considered as the only independent variable to predict the practical success of PCI. Chance of success in patients with AF was 2% less than others (odds ratio (OR): 0.02; 95% confidence interval (CI): 0.00 - 0.54; P = 0.018). Also, according to the multivariate correlation test results, aging independently does not affect the success of PCI and practical chance of success or failure of PCI will not be affected by old age (Table 4).
Click to view | Table 4. Multivariate Logistic Correlation Test for Practical Success of PCI |
Based on Pearson’s and Spearman correlation results, older age, a history of CVA, the risk of HF and AF have a significant but weak correlation with the practical success of PCI. The strongest factor associated with the practical failure of PCI is the incidence of AF. Aging, especially aged 75 years, has a weak significant relationship with the practical success of PCI, so that along with increasing age, the success rate will be decreased (Table 5).
Click to view | Table 5. Results of Spearman Correlation Test of the Relationship of Each Variable With the Practical PCI Success |
| Discussion | ▴Top |
In the study conducted by Pourhosseini et al, the study population was only 1.2% of the patients above 80 years of age to 17 years, who were undergoing PCI in angioplasty in Tehran Heart Center [12]. Percentage of population aged over 80 years in our study compared to study conducted by Pourhosseini et al indicates that perhaps in recent years, in addition to the results of several clinical trials of more advantage of early aggressive approach compared to conservative supportive therapies in older adults [8], the overall sensitivity of interventional cardiologists to perform the aggressive intervention and selecting treatment approach of PCI in elderly patients has been less.
In the present study, the concurrent prevalence of coronary multi-vessel stenosis in the elderly was more and elderly patients were with comorbidities more than non-elderly. The prevalence of diabetes, dyslipidemia, and smoking in the age group below 70 years was more, while the more elderly were with high blood pressure, HF, CKD and AF and lower percentage of LVEF. In a similar study, Feldman et al showed that the risk of high blood pressure, HF, kidney failure and multi-vessel coronary disease in elderly patients above 87 years has been the most common; on the other hand, the prevalence of smoking in younger patients has been significantly higher than the elderly [13]. In a similar study, Feldman et al showed that the risk of high blood pressure, hf, kidney failure and multi-vessel coronary disease in elderly patients above 87 years has been the most common; on the other hand, the prevalence of smoking in younger patients has been significantly higher than the elderly [13].
In a 7-year prospective study conducted by Cathy et al, in total, 11.1% of patients were over 70 years old and the number of elective PCI in the seventh year increased up to twofold the first year, and annually the number of elderly patients was added. The prevalence of multi-vessel disease and multiple comorbidities and a history of MI and CABG were higher in elderly patients. Of course, similar to our study, the prevalence of diabetes was not a significant difference in the two age groups. On the other hand, unlike the present study, the prevalence of smoking in the elderly and non-elderly patients was almost same and every year, in both age groups decreased significantly. The study also reveals that a significant increase in the number of PCIs during the time indicates the change of attitude in selecting the patient. In fact, over time, the vascular intervention by the PCI approach has had more outbreaks among the elderly due to the adverse clinical conditions and the more severity of coronary atherosclerosis lesions; in addition, compared to the former, younger patients with vascular lesions tend to treat with PCI more than medical treatment [14].
According to the results of multiple trials of better prognosis and improved clinical outcomes for angioplasty using DES [7], the experts’ approach in 98% of cases in this study has been the use of DES in patients. In a similar study, a stent was used in 91.9% that the DES includes 43.3% of the stents and its use in the elderly has been clearly less than younger patients [12]. While the success rate of primary PCI was similar in the two age groups, elderly patients showed a higher rate of the practical failure of the PCI. Although the rate of ischemic attacks and death in the elderly was more than non-elderly patients, the incidence of MACE showed a very poor with aging. The length of stay, renal complications, cardiac arrhythmia and significant localized bleeding in the elderly were seen significantly higher than in patients under 70 years. Among the patients, the elderly due to more complex vascular lesions and weaker clinical situations and narrower adjustment capacity are more prone to cardiovascular major side events and minor complications. Our study had results similar to Miura et al’s study of the clinical outcomes of in-hospital PCI in older adults less than 67 years, despite 22.9% of elderly patients that showed a success rate of angiography in elderly patients is no different from non-elderly patients, but the practical success of PCI in the elderly is significantly less. It was also observed in the rate of MACE and mortality during hospitalization in the elderly is clearly higher than younger patients [15].
Based on the CADILLAC trial, despite more risk factors in elderly people, which represent prognosis for the patient, the success rate of PCI is with similar results in elderly and younger patients. However, aging is independently in connection with prognosis for patient survival outcome in the short term or long term [16]. Also, Voudris et al studied 69 patients above 70 years and 333 patients younger than 70 years and saw that the practical success of PCI did not differ between the two groups [17].
In another study, the researchers estimated that PCI failure rate increases along with the increase of age, and mortality in patients older than 80 years, who were faced with the failure of PCI, is significantly more. In fact, the increase of mortality rates both during hospitalization and in the long-term was associated with increasing age. In multivariate analysis, successful PCI was associated with the improved clinical outcomes in all age groups. In general, however, in the first, the PCI failure, adverse events, and mortality were observed more in the elderly, but the prognosis in cases of successful PCI of all ages was similar and acceptable [11].
In their study, Nouhi et al evaluated clinical outcomes of PCI, and found that the majority of patients had at least one of the risk factors for atherosclerosis, including hypertension as a common risk factor. However, the only factor associated with the practical failure of the PCI was the adverse events and mortality both during hospitalization and during follow-up of patients with cardiogenic shock on admission [18]. Our study showed that aging alone in no way affects the occurrence of PCI practical failure. While the PCI ending in failure was significantly higher in elderly patients, the strong underlying factors for the higher rate of failure, AF, and heart failure are more common in elderly patients. In general, the results showed that the incidence of AF in the patients is the only independent factor affecting the practical failure of the PCI, and is associated the practical failure of PCI more than any other factor, so that the outcome of PCI in 25% of patients was not successful. In addition, it seems that a history of CVA and HF increased failure rates in patients. Also aging is not a strong factor for the prediction of in-hospital side effects and increases only an 8% chance of side effects (major and minor) in the patients, and the presence of HF, chronic renal failure, history (CVA and risk of AF), increase the risk of complications in patients more than age.
According to the studies conducted by Miura and Pourhosseini like the present study, aging is not a predictive factor of practical failure of PCI and the occurrence of MACE [4, 12]. Pourhosseini and colleagues demonstrated that the strongest predictive factor for PCI failure is type of coronary lesions, so more chronic, more serious and more widespread atherosclerotic lesions more than aging are risky for PCI.
Study limitations
Although we tried to record and collect proper data about a momentous number of patients with CAD undergoing PCI by various experts in a health facility over a year, to assess the independent effects of age and other factors on the success or failure of the PCI and its complications still needs larger population and larger sample size. On the other hand, however, in patients entering in this study in 1 year in succession, but in all cases of PCI, deciding how to do it or, if necessary, perform angioplasty on a few stages for high-risk patients, was the prerogative of the relevant specialist; as a result, there is a possibility of bias in patient selection and PCI. Furthermore, given that in this center, PCI is done only for elective, the results cannot be generalized to emergency cases of PCI and to assess the effect of age on the success or failure of PCI and its complications has been limited to selective and conservative terms in performing PCI.
Conclusion
While the results of the PCI during hospitalization showed a failure rate of PCI and the incidence of major adverse cardiovascular complications and complications leading to hospitalization longer in elderly patients significantly is higher than younger ages, but overall aging does not increase chances of practical failure of the PCI and the incidence and to be complicated, and prognosis of the patients, most of all, is affected by underlying diseases and CAD in his or her situation. In addition, the accepted hospital prognosis, according to multiple internal and external trials, in the long term, the elderly profit favorable clinical outcomes of treatment by PCI approach, especially using DES, more than the maximum optimal pharmaceutical treatment. So, the decision to conduct a PCI based on the patient’s age does not seem to be logical.
Recommendations
In the study of prognosis of invasive interventions such as PCI, to strengthen the scientific foundations of research, in addition to the more accurate and more comprehensive follow-up of patients, taking multiple statistical populations concentratedly and subsequently more size of the sample, is very important. So for the guidance of experts and relevant authorities and to provide strategic outcomes to health centers in the country and possibility of citation of results of internal research by other experts, to further explore the implications of PCI in elderly patients in our country, seems necessary.
Acknowledgments
This project would never have been possible without the support and guidance of various people at the Qom University of Medical Science and Health Services. This article is derived from MD thesis by “In-hospital Clinical outcomes of PCI in elderly patients of Qom Shahid Beheshti Hospital” title and by “MUQREC.1393.136” registration number.
| References | ▴Top |
- Noroozian M. The elderly population in iran: an ever growing concern in the health system. Iran J Psychiatry Behav Sci. 2012;6(2):1-6.
pubmed - Farokhnezhad Afshar P, Asgari P, Shiri M, Bahramnezhad F. A review of the Iran's elderly status according to the census records. Galen Med J 2016;5(1):6.
- Antman E LJ. Ischemic Heart Disease. In: Kasper D HS, Jameson L, Fauci A, Longo D, Loscalzo J. Harrison's Principles of Internal Medicine. 19th edn. New York: McGraw-Hill Education; 2015: p. 1578-1593.
- Miura T, Soga Y, Aihara H, Yokoi H, Iwabuchi M. Prevalence and clinical outcome of polyvascular atherosclerotic disease in patients undergoing coronary intervention--reply. Circ J. 2013;77(5):1349.
doi pubmed - Athyros VG, Katsiki N, Karagiannis A. Prevalence and clinical outcome of polyvascular atherosclerotic disease in patients undergoing coronary intervention. Circ J. 2013;77(5):1348.
doi pubmed - Miura T, Soga Y, Doijiri T, Aihara H, Yokoi H, Iwabuchi M, Nobuyoshi M. Prevalence and clinical outcome of polyvascular atherosclerotic disease in patients undergoing coronary intervention. Circ J. 2013;77(1):89-95.
doi pubmed - Fox KA, Poole-Wilson P, Clayton TC, Henderson RA, Shaw TR, Wheatley DJ, Knight R, et al. 5-year outcome of an interventional strategy in non-ST-elevation acute coronary syndrome: the British Heart Foundation RITA 3 randomised trial. Lancet. 2005;366(9489):914-920.
doi - Pfisterer M, Buser P, Osswald S, Allemann U, Amann W, Angehrn W, Eeckhout E, et al. Outcome of elderly patients with chronic symptomatic coronary artery disease with an invasive vs optimized medical treatment strategy: one-year results of the randomized TIME trial. JAMA. 2003;289(9):1117-1123.
doi pubmed - Roberts JK, Rao SV, Shaw LK, Gallup DS, Marroquin OC, Patel UD. Comparative efficacy of coronary revascularization procedures for multivessel coronary artery disease in patients with chronic kidney disease. Am J Cardiol. 2017;119(9):1344-1351.
doi pubmed - Khawaja MZ, Wang D, Pocock S, Redwood SR, Thomas MR. The percutaneous coronary intervention prior to transcatheter aortic valve implantation (ACTIVATION) trial: study protocol for a randomized controlled trial. Trials. 2014;15:300.
doi pubmed - Fach A, Bunger S, Zabrocki R, Schmucker J, Conradi P, Garstka D, Fiehn E, et al. Comparison of Outcomes of Patients With ST-Segment Elevation Myocardial Infarction Treated by Primary Percutaneous Coronary Intervention Analyzed by Age Groups (<75, 75 to 85, and >85 Years); (Results from the Bremen STEMI Registry). Am J Cardiol. 2015;116(12):1802-1809.
doi pubmed - Poorhosseini H, Mousavi M, Nematipour E, Kassaian SE, Salarifar M, Alidoosti M, Hajizeinali A, et al. Success rate, procedural complications and clinical outcomes of coronary interventions in octogenarians: a case-control study. J Tehran Heart Cent. 2011;6(3):126-133.
pubmed - Feldman DN, Gade CL, Slotwiner AJ, Parikh M, Bergman G, Wong SC, Minutello RM, et al. Comparison of outcomes of percutaneous coronary interventions in patients of three age groups (<60, 60 to 80, and >80 years) (from the New York State Angioplasty Registry). Am J Cardiol. 2006;98(10):1334-1339.
doi pubmed - Johnman C, Oldroyd KG, Mackay DF, Slack R, Pell AC, Flapan AD, Jennings KP, et al. Percutaneous coronary intervention in the elderly: changes in case-mix and periprocedural outcomes in 31,758 patients treated between 2000 and 2007. Circ Cardiovasc Interv. 2010;3(4):341-345.
doi pubmed - Miura T, Miyashita Y, Motoki H, Shimada K, Kobayashi M, Nakajima H, Kimura H, et al. In-hospital clinical outcomes of elderly patients (>/=80 years) undergoing percutaneous coronary intervention. Circ J. 2014;78(5):1097-1103.
doi pubmed - Wenaweser P, Ramser M, Windecker S, Lutolf I, Meier B, Seiler C, Eberli FR, et al. Outcome of elderly patients undergoing primary percutaneous coronary intervention for acute ST-elevation myocardial infarction. Catheter Cardiovasc Interv. 2007;70(4):485-490.
doi pubmed - Voudris VA, Skoularigis JS, Malakos JS, Kourgianides GC, Pavlides GS, Manginas AN, Kolovou GD, et al. Long-term clinical outcome of coronary artery stenting in elderly patients. Coron Artery Dis. 2002;13(6):323-329.
doi pubmed - Noohi F, Hashemi I, Sanati HR, Peighambari MM, Kiavar M, Maadani M, Bassiri HA, et al. In-hospital and six-month outcomes of elderly patients undergoing primary percutaneous coronary intervention for acute ST-elevation myocardial infarction. ARYA Atheroscler. 2016;12(1):28-34.
pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.