

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Original Article
Volume 10, Number 4, August 2019, pages 216-222
A Simplified Risk Scoring System to Predict Mortality in Cardiovascular Intensive Care Unit
Hendry Purnasidha Bagaswotoa, b, Nahar Taufiqa, Budi Yuli Setiantoa
aCardiology and Vascular Medicine Department of Medical, Public Health, and Nursing Faculty Universitas Gadjah Mada/Sardjito General Hospital Yogyakarta, Jl. Farmako, Senolowo, Sekip Utara, Kec. Depok, Kabupaten Sleman, Daerah Istimewa Yogyakarta 55281, Indonesia
bCorresponding Author: Hendry Purnasidha Bagaswoto, Cardiology and Vascular Medicine Department of Medical, Public Health, and Nursing Faculty Universitas Gadjah Mada/Sardjito General Hospital Yogyakarta, Jl. Farmako, Senolowo, Sekip Utara, Kec. Depok, Kabupaten Sleman, Daerah Istimewa Yogyakarta 55281, Indonesia
Manuscript submitted May 21, 2019, accepted May 30, 2019
Short title: Scoring System to Predict Mortality in CICU
doi: https://doi.org/10.14740/cr884
| Abstract | ▴Top |
Background: Cardiovascular intensive care unit (CICU) is an area with high mortality rates globally. The prediction of inpatients mortality risk at CICU needs a simplified scoring systems. Hence, this study aims to analyze the predictors for in-hospital mortality of patients whom hospitalized at CICU of Sardjito General Hospital Yogyakarta and to create a mortality risk score based on the results of this analysis.
Methods: Data were obtained from SCIENCE (Sardjito Cardiovascular Intensive Care) registry. Outcomes of 595 consecutive patients (mean age 59.92 ± 13.0 years) from January to November 2017 were recorded retrospectively. Demography, risk factor, comorbidities, laboratory result and other examinations were analyzed by multivariate logistic regression to create two models of scoring system (probability and cut-off model) to predict in-hospital mortality of any cause.
Results: A total of 595 subjects were included in this research; death was found in 55 patients (9.2%). Multiple logistic regression analysis showed some variables that became independent predictor of mortality, i.e. age ≥ 60 years, pneumonia, the use of ventilator machine, and increased of serum glutamate-pyruvate transaminase level, an increased of creatinine level and an ejection fraction < 40%. Receiver operating characteristic (ROC) curve analysis showed a cut-off model scoring system with score 3 to 9 predicting mortality compared to score 0 - 2. This model yielded sensitivity of 80% and specificity 74%. While the probability scoring system (score 0 to 9) showed that the higher the score, the higher the mortality probability (e.g. the mortality of patient with score 2 is 5.27%; while the mortality of patient with score 8 is 87.5%).
Conclusions: Scoring system derived from this study can be used to predict the in-hospital mortality of patients whom hospitalized in our CICU and show a favorable sensitivity and specificity result.
Keywords: Scoring system; In-hospital mortality; CICU patients
| Introduction | ▴Top |
Cardiovascular disease is one of the main causes of death worldwide, and an important etiology of some morbidity in life. For majority of cardiovascular diseases, early diagnosis (within minutes) and early intervention can be independent outcome defining factors. Expert clinicians and adequate health facilities in the health care center are needed to manage these critical patients [1].
Scoring systems are used to assess disease severity of patients in the critical care unit. This scoring system mainly use the patient’s data in the first 24-h period after the patient came to the critical care unit to predict short-term outcome, such as in-hospital mortality rate [2].
Most of the scoring systems used for patient management in the intensive care unit (ICU) are complex and needed to be updated regularly. Acute Physiology and Chronic Health Evaluation (APACHE) and Simplified Acute Physiology Score (SAPS) are two most frequent scoring systems used by clinicians [2]. These scoring systems (APACHE II, IV and SAPS III) have the same sensitivity and specificity in predicting ICU patients mortality [3].
Most of the available scoring systems are used to predict the ICU patients mortality, whereas the scoring systems specifically for cardiovascular intensive care unit (CICU) patients have not yet adequately developed. This is essential as acute coronary syndrome, acute or chronic heart failure, cardiogenic shock, valvular heart disease, arrhythmia and pulmonary embolism highly contribute to mortality rate in the CICU [2, 4].
Some predictors included in the APACHE score are comorbidity factors, resuscitation in the beginning of inpatient, the use of mechanic ventilator, and so on [2]. Some studies show that there are other predictors of mortality especially in patients who undergo open heart surgeries; body mass index > 27 kg/m2, glomerulus filtration rate < 50 mL/min, New York Heart Association (NYHA) class IV heart failure and systolic pulmonary arterial pressure > 55 mm Hg [5].
The aim of this study is to analyze characteristics that can be used as predictors of mortality which in the future can be developed into a scoring system to predict mortality rate at CICU of Sardjito General Hospital.
| Materials and Methods | ▴Top |
This is a cross sectional study aiming to analyze factors which can be used to predict patient mortality at CICU and to develop a scoring system subsequently. All patients at CICU of Sardjito General Hospital Yogyakarta were collected consecutively from January until October 2017. Inclusion criteria include study participants aged > 18 years old and signed a informed consent to participate in the study. Demographic data (age, gender and the patient risk factors), clinical data (patient comorbidities), laboratory examination (routine blood test, renal function, liver function and blood sugar) and echocardiography (ejection fraction and right ventricular function (tricuspid annular plane systolic excursion (TAPSE)) were obtained.
The independent variables in this study are all factors that can predict mortality whilst the dependent variable is mortality regardless the etiology. However, the mortality data are limited by only those happened during treatment at the CICU.
A bivariate analysis was used to analyze the association between predicting factors and mortality. Chi-square test was chosen to analyze the correlation with Fisher’s test as an alternative test. Furthermore, a multivariate analysis was undertaken by taking variables in the bivariate analysis with P < 0.25. Then a logistic regression was used with stepwise backward method. B and SE score from SPSS were then added to scoring system using multivariate analysis. There are two scoring systems derived from this analysis: 1) Probability; and 2) Cut-off scoring system which based on receiver operating characteristic (ROC) curve. The previous scoring system would be validated to some samples to find out their diagnostic value. All data analysis was conducted by SPSS ver.16 program.
Other essential informations needed from the research participants were taken from the medical record or direct anamnesis with the participants. Data sampling was done with non-probability sampling.
Research ethic
The study was conducted according to the Institutional Review Board guidelines at the Faculty of Medicine, Public Health, and Nursing Universitas Gadjah Mada/Sardjito General Hospital on human subjects, and complies with the Helsinki Declaration. Each participant enrolled in the study has been given a thorough explanation based on informed consent.
| Results | ▴Top |
Of 595 participants enrolled during the study, mean age in this population is 60 years old and majority of the patient is male (71.9%). The most common diagnosis is acute coronary syndrome (69.9%). ST-elevation acute myocardial infarction (STEAMI) was found more frequent compared to acute non-ST-elevation acute myocardial infarction (NSTEAMI) with 69.7% and 30.3%, respectively. Mortality event is found in 55 patients (9.2%) regardless of the etiology (Table 1).
 Click to view | Table 1. Baseline Characteristics of the Research Subject |
Bivariate analysis showed significant difference between some predictors that affecting the mortality event in this study. These are pneumonia, diabetes mellitus, the use of ventilator, hemoglobin level < 10 g/dL, creatinine level > 1.5 mg/dL, random blood glucose > 200 mg/dL, serum glutamic oxaloacetic transaminase (SGOT) and serum glutamic pyruvic transaminase (SGPT) > 50 U/L, decreased right ventricular function with TAPSE < 17 mm and left ventricle ejection fraction < 40% (Table 2).
Click to view | Table 2. Baseline Characteristic of the Research Subject (Survivor versus Non-Survivor) |
Multivariate analysis also showed some factors could be independent predictors of mortality, those are age ≥ 60 years old (odds ratio (OR): 1.97), pneumonia (OR: 2.51), the use of mechanical ventilator (OR: 20.98), creatinine level > 1.5 mg/dL (OR: 2.97), SGPT level > 50 U/L (OR: 1.42) and an ejection fraction < 40% (OR: 2.21) (Table 3).
Click to view | Table 3. Multivariate Analysis of Factors Predicting Mortality (N = 595 Patients) |
Each of the independent predictors was assessed to create a calculation for CICU scoring system (Table 4).
Click to view | Table 4. Assessment of the Score Value From Each Independent Predictor Factor |
The first scoring system model is based on the probability to have mortality event with minimum score of +1 and a maximum score of +9 (Table 4).
Regression test was used to form a scoring system based on the probability of mortality event. For example, the probability that the patient would experience mortality is 75.9% if a patient has a total score of 7 (Table 5).
Click to view | Table 5. Scoring System Based on Patient’s Probability on Mortality Event |
The second scoring system model is based on cut-off point in the ROC curve analysis. The ROC statistical method is derived from trading off between sensitivity and specificity in some alternative cut-off points presented as a graphic (Fig. 1, Table 6).
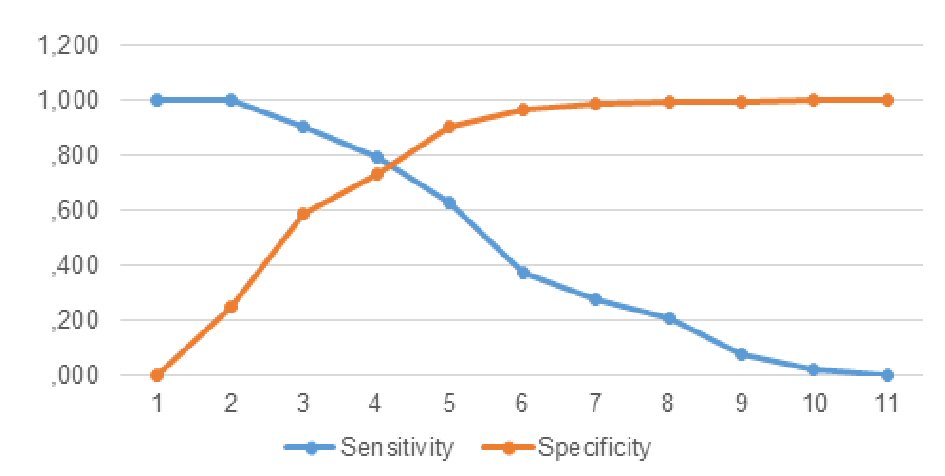 Click for large image | Figure 1. Sensitivity and specificity graph based on ROC analysis. |
Click to view | Table 6. Sensitivity and Specificity of Each Graphic Point Towards Patient’s Probability to Experience Mortality Event |
From a cut-off analysis between Figure 1 and Table 6, a cut-off point of 4 was taken. Thus, a score between +3 and +9 has a higher chance to have an outcome of death than a score between +1 and +2. This scoring system has 80% sensitivity with 74% specificity to predict a mortality event.
| Discussion | ▴Top |
This study collected 595 participants from January to October 2017 at CICU of Sardjito General Hospital. During that period, acute coronary syndrome (69.9%) was identified as the most common diagnosis. Of acute coronary syndrome patients, STEAMI was the majority cause (69.7%). Other diagnoses found at CICU are arrhythmia (14.1%), followed by post-heart surgery patient (4.7%), worsening of heart failure (4.2%), peripheral vascular disease (3.7%), and other causes (3.5%).This result looks similar compared to previous study done by Dogan et al [6] who reported that 65% CICU patients was diagnosed by acute coronary syndrome and 43.4% of them was STEAMI. Other study [7] also showed that acute coronary syndrome was the main diagnosis for inpatients in the ICU (57%) with 46.2% STEAMI and 53.7% NSTEAMI. The result was followed by systolic heart failure (6.2%), bradycardia (5.6%), cardiac arrest (4.6%) and atrial fibrillation (3.6%).
Fifty-five patients (9.2%) died during the study and mostly due to cardiogenic and septic shock. Patient mortality rate between previous studies are different (12.7% [6], 5.6% [7], 13% [8] and 7-8% [9]). The leading cause of death is also varied like cardiogenic shock, sepsis and respiratory failure [7].
Some studies have analysed mortality predictor factors which were recorded at patient’s entry to CICU such as hypotension, tachycardia, low oxygen saturation, increased blood urea level, blood sugar level, magnesium, liver enzyme, troponin and B-type natriuretic peptide [7]. Our study showed that factors that can work as a predictor of mortality include pneumonia, diabetes mellitus, the use of mechanical ventilator, haemoglobin level < 10 g/dL, creatinine level > 1.5 mg/dL, random blood sugar > 200 mg/dL, SGOT and SGPT level > 50 U/L, decreased of right ventricular function with TAPSE < 17 mm and reduced ejection fraction < 40%.
Multivariate analysis shows factors can act as an independent predictor of mortality, which are age ≥ 60 years (OR: 1.97), presence of pneumonia as comorbid factor (OR: 2.51), mechanical ventilator utilization (OR: 20.98), creatinine level > 1.5 mg/dL (OR: 2.97), SGPT level > 50 U/L (OR: 1.42) and also ejection fraction < 40% (OR: 2.21).
In our study, age ≥ 60 years old is an independent predictor of mortality. The findings of other studies found age as a predictor factor of mortality. There is a significant difference between mean age of the patient that has an outcome of death compare to the other group with better outcome (75 versus 66.9; P < 0.001) [7]. Studies conducted found that patient with age ≥ 65 years old have a significantly higher mortality risk when treated in the ICU (HR: 1.81 with CI 1.49 - 2.19; P < 0.001) [10].
Pneumonia is an independent predictor of mortality in our study that has OR of 2.51. Community acquired pneumonia (CAP) is a disease which is closely related to an increase in mortality rate. The mortality rate of CAP in inpatients during the period is 12%, and can reach more than 30% if the patient is treated in the ICU [11]. From a study which take a population of > 2,000 patient with diagnosis of CAP, 75% of the patient treated in the ward of the hospital with age ≥ 65 years old have a higher mortality compare to younger patient population. Age is an independent risk factor of death in pneumonia patients because an elderly patient usually has a more advance stage of the disease at the time of admission. The clinical symptom of pneumonia in the elderly is not clearly visible, vital sign parameter usually does not show an abnormal result compare to the younger patients. In addition, the doctor and patient’s family can overlook pneumonia at early diagnosis [12].
Utilization of mechanical ventilation acts as an independent predictor of mortality in our study with the highest OR associated with mortality event (OR: 20.98). One study which analyse predictor of mortality in the ICU patient also found that utilization of mechanical ventilator correlate with mortality event 11.7% [7]. Other study that assess outcome of patient ≥ 65 years old whom is treated in the ICU, also found that utilization of mechanical ventilator can become an independent predictor of mortality event with HR of 2.74 (CI: 2.00 - 3.76; P < 0.001) [10]. In another study, from a total of 1,115 ICU patients using a mechanical ventilator, the mortality rate is found to be 51% (564 patients). Further analysis shows that age is one independent predictor of mortality in this study (HR: 1.01 with CI: 1.004 - 1.014; P < 0.001) [13].
Laboratory examination results that can work as an independent predictor of mortality event in our study is increase in creatinine level > 1.5 mg/dL (OR: 2.97) and SGPT > 50 U/L (OR: 1.42). Decrease in renal function is also found to be associated with mortality and can be an independent predictor of mortality in ICU patient using a mechanical ventilator (HR: 1.29 with CI: 1.06 - 1.56; P = 0.011) [13]. Whereas, an increase in transaminase enzyme is found to correlated with a higher chance of mortality in another study, which shows that mean SGOT is higher in non-survivor group compared to survivor group of patient (74.9 U/L versus 460 U/L; P = 0.000), this result is similar to SGPT level (52.8 U/L versus 280.8 U/L; P = 0.000) [7]. But our study found that SGOT is not an independent predictor of mortality although bivariate analysis shows that increase in SGOT > 50U/L has a significant value with OR of 2.43 (CI: 1.447 - 4.068; P = 0.001). Result from a study which analysed the influence of an increase in enzyme transaminase level to cardiovascular mortality risk from 2,061 subjects aged 50 - 99 years old observed that an increase of SGPT level > 40 U/L (on male) and SGPT > 31 U/L (on female) have a higher mortality risk regardless of the etiology of death. In addition, age remains a key factor where the risk is lower in younger subject population (age ≤ 59 years old, HR: 0.46; 95% CI: 0.06 - 3.49), but will increase with age; age 60 - 69 years old (HR: 1.05; 95% CI: 0.53 - 2.07), age 70 - 79 years old (HR: 1.54; 95% CI: 0.81 - 2.93), and age ≥ 80 years old (HR: 3.53; 95% CI: 1.55 - 8.04). Meanwhile, cardiovascular mortality risk also increases with age; age 70 - 79 years old (HR: 3.15; 95% CI: 1.37 - 7.23) and age ≥ 80 years old (HR: 6.86; 95% CI: 2.44 - 19.3). SGPT enzyme has a role as a specific inflammation enzyme in the liver thus an increase in SGPT enzyme level indicated a severe inflammation process that can affect mortality event [14].
Study that evaluated an abnormality in liver function test on 263 patients with critical disease found that the use of mechanical ventilator, hemofiltration and hypotension on the first 48 h correlated with abnormality of SGPT level on the third day. Abnormal SGPT level was associated with an increase in mortality risk in 30 days period (OR: 2.7; CI: 1.2 - 6.0) [15].
We also found that fraction ejection value < 40% is an independent predictor of mortality with OR of 2.21 (CI: 1.077 - 4.554; P = 0.031). Mortality in heart failure patient based on some studies is inversely related with left ventricle systolic function. Fraction ejection level is considered as the strongest prognosis factor that affecting poor outcome in heart failure patient [16]. Presence of systolic heart failure is a contributing factor to mortality event in another study that takes a 956 patients population treated in the ICU. In that study mortality event was found in 59 patients (6.1%). Systolic heart failure is found more frequently in non-survivor group compared to survivor group (30.5% versus 14.7%; P = 0.001) [7].
Limitations
This scoring system is still limited to apply to our hospital. Further research is needed to validate this scoring system when applied to CICU at other hospitals.
Conclusions
The scoring system developed from this study can be utilized to predict mortality event at CICU of Sardjito General Hospital, and showed a favorable sensitivity and specificity result. Factors that work as independent predictor of mortality in this study are age ≥ 60 years old, presence of pneumonia as a comorbid factor, utilization of mechanical ventilation, increase in creatinine level > 1.5 mg/dL, SGPT > 50 U/L, and ejection fraction level < 40%.
Acknowledgments
None to declare.
Financial Disclosure
No funding or sponsorship was received for this study or publication of this article.
Conflict of Interest
The authors declare that they have no competing interest.
Informed Consent
All patients provided informed consent.
Author Contributions
Authors whose names appear on submission have contributed sufficiently to the design of the study, acquiring, analysing, and interpreting the data.
Abbreviations
OR: odds ratio; HR: hazard ratio; CICU: cardiovascular intensive care unit; ICU: intensive care unit; APACHE: Acute Physiology and Chronic Health Evaluation; SAPS: Simplified Acute Physiology Score; NYHA: New York Heart Association; TAPSE: tricuspid annular plane systolic excursion; STEAMI: ST-elevation acute myocardial infarction; NSTEAMI: Non-ST-elevation acute myocardial infarction; SGPT: serum glutamic pyruvic transaminase; SGOT: serum glutamic oxaloacetic transaminase; ROC: receiver operating characteristic
| References | ▴Top |
- Price S, Tubaro M, Vranckx P, Vrints C. Intensive and acute cardiac care: an introduction. In: Tubaro, M, Vranckx, P, Price S, Vrints C. editors. The ESC textbook of intensive and acute cardiovascular care. Second Edition. Oxford University Press; 2015:3-4.
doi - Killeen TK, Back SE, Brady KT. Implementation of integrated therapies for comorbid post-traumatic stress disorder and substance use disorders in community substance abuse treatment programs. Drug Alcohol Rev. 2015;34(3):234-241.
doi pubmed - Evran T, Serin S, Gurses E, Sungurtekin H. Various scoring systems for predicting mortality on intensive care unit. Niger J Clin Pract. 2016;19:530-534.
doi pubmed - Weiner SD, Rabbani LE. Cardiac intensive care unit admission criteria. In: Jeremias A, Brown DL. Cardiac Intensive Care. 2nd Edition. Philadelphia: Saunders Elsevier; 2010:25-32.
doi - Gatti G, Perrotti A, Obadia JF, Duval X, Iung B, Alla F, Chirouze C, et al. Simple scoring system to predict in-hospital mortality after surgery for infective endocarditis. J Am Heart Assoc. 2017;6(7):e004806.
doi - Dogan S, Dursun H, Can H, Ellidokuz H, Kaya D. Long-term assessment of coronary care unit patient profile and outcomes: analyses of the 12-years patient records. Turk J Med Sci. 2016;46(3):801-806.
doi pubmed - Ratcliffe JA, Wilson E, Islam S, Platsman Z, Leou K, Williams G, Lucido D, et al. Mortality in the coronary care unit. Coron Artery Dis. 2014;25(1):60-65.
doi pubmed - Teskey RJ, Calvin JE, McPhail I. Disease severity in the coronary care unit. Chest. 1991;100(6):1637-1642.
doi pubmed - Katz JN, Shah BR, Volz EM, Horton JR, Shaw LK, Newby LK, Granger CB, et al. Evolution of the coronary care unit: clinical characteristics and temporal trends in healthcare delivery and outcomes. Crit Care Med. 2010;38(2):375-381.
doi pubmed - Mukhopadhyay A, Tai BC, See KC, Ng WY, Lim TK, Onsiong S, Ee S, et al. Risk factors for hospital and long-term mortality of critically ill elderly patients admitted to an intensive care unit. Biomed Res Int. 2014;2014:960575.
doi pubmed - Brito V, Niederman MS. Predicting mortality in the elderly with community-aquired pneumonia: should we design a new car or set a new "Speed Limit"? Thorax. 2010;65:943-944.
doi pubmed - Kothe H, Bauer T, Marre R, Suttorp N, Welte T, Dalhoff K, Competence Network for Community-Acquired Pneumonia study g. Outcome of community-acquired pneumonia: influence of age, residence status and antimicrobial treatment. Eur Respir J. 2008;32(1):139-146.
doi pubmed - Fialkow L, Farenzena M, Wawrzeniak IC, Brauner JS, Vieira SR, Vigo A, Bozzetti MC. Mechanical ventilation in patients in the intensive care unit of a general university hospital in southern Brazil: an epidemiological study. Clinics (Sao Paulo). 2016;71(3):144-151.
doi - Mahady SE, Wong G, Turner RM, Mitchell P, Macaskill P, Craig JC, George J. Elevated liver enzymes and mortality in older individuals: a prospective cohort study. J Clin Gastroenterol. 2017;51(5):439-445.
doi pubmed - Thomson SJ, Cowan ML, Johnston I, Musa S, Grounds M, Rahman TM. 'Liver function tests' on the intensive care unit: a prospective, observational study. Intensive Care Med. 2009;35(8):1406-1411.
doi pubmed - Ponikowski P, Jankowska EA, Banasiak W. Prognosis in diastolic heart failure. In: Smiseth OA, Tendera M. Diastolic heart failure. London: Springer-Verlag, 2008:213-220.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.