

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Original Article
Volume 10, Number 5, October 2019, pages 293-302
This article has been retracted in Vol. 15, No. 4, Aug 2024.
Sacubitril/Valsartan Therapy for 14 Months Induces a Marked Improvement of Global Longitudinal Strain in Patients With Chronic Heart Failure: A Retrospective Cohort Study
Renato De Vecchisa, d, Andrea Pacconeb, Marco Di Maioc
aPreventive Cardiology and Rehabilitation Unit, DSB 29 “S. Gennaro dei Poveri Hospital”, via S.Gennaro dei Poveri 25, 80136 Naples, Italy
bDepartment of Cardiology, University of Bari “Aldo Moro”, Bari, Italy
cDepartment of Cardiology, University of Campania “Luigi Vanvitelli”, 80138 Naples, Italy
dCorresponding Author: Renato De Vecchis, Preventive Cardiology and Rehabilitation Unit, DSB 29 “S. Gennaro dei Poveri Hospital”, via S.Gennaro dei Poveri 25, 80136 Naples, Italy
Manuscript submitted July 12, 2019, accepted August 16, 2019
Short title: Sacubitril/Valsartan Therapy for CHF
doi: https://doi.org/10.14740/cr910
| Abstract | ▴Top |
Background: Clinical efficacy of sacubitril/valsartan administered for the recommended indication of chronic heart failure (CHF) patients with New York Heart Association (NYHA) classes II-III appears to be higher than one would expect based on the drug-induced variations of the left ventricular ejection fraction (LVEF). More thorough investigations with the use of indicators of longitudinal systolic function have been therefore recommended to verify whether a part of the clinical improvement achieved with the use of sacubitril/valsartan could be supported by a reverse remodeling ensuing from changes other than a simple LVEF increase.
Methods: In the present retrospective cohort study, which collected the pertinent data from two centers devoted to clinical management of outpatients with CHF and dating back to the years 2017 and 2018, we separated patients treated with sacubitril/valsartan from those treated with conventional medical therapy, including angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers (ARBs). For the rest, the therapies practiced in the two groups, patients under sacubitril/valsartan and controls, were almost identical, including similar doses of beta-blockers and mineralocorticoid receptor antagonists (MRAs) in the two cohorts, plus loop diuretics, with the latter administered at variable doses. The endpoints were the variations of LVEF and global left ventricular longitudinal strain (GLS) over a study period not shorter than 1 year.
Results: One hundred thirty-two patients were collected within our retrospective cohort study, of whom 44 were treated with sacubitril/valsartan and 88 were subjected to conventional therapy. All patients were marked by heart failure with reduced (LVEF ≤ 40%) left ventricular ejection fraction (HFREF). The mean duration of the retrospective observation period was 14 ± 3 months. In controls, LVEF was improved after a year of therapy from 38.071 ± 5.445% (mean ± standard deviation) to 41.595 ± 5.282%. On the contrary, no significant improvement in the controls could be identified for the GLS, from -12.059 ± 4.016% to -12.250 ± 4.287%. In analogy with controls, patients assigned to sacubitril/valsartan showed a significant increase in LVEF after 1 year of treatment from 39.714 ± 4.789% to 42.119 ± 5.683% (P < 0.001). However, differently from the controls, sacubitril/valsartan group exhibited a significant improvement in GLS from -10.142 ± 3.080% to -18.238 ± 7.284% (P < 0.001).
Conclusions: The present retrospective cohort study demonstrated that the use of sacubitril/valsartan for HFREF patients, extended for a mean duration of 14 months, yields a significant improvement in the echocardiographic parameters of systolic function along the transverse (LVEF) and longitudinal (GLS) axis. For the GLS in particular, a clear superiority emerges in comparison with conventional therapy including ACE inhibitor or ARBs. From these data, the hypothesis could be derived of a possible useful role of sacubitril/valsartan also for the therapy of HFpEF. In this regard, more exhaustive clarifications ensuing from the ongoing randomized controlled trials (RCTs) are eagerly awaited.
Keywords: Sacubitril/valsartan; Global longitudinal strain; Clinical outcomes
| Introduction | ▴Top |
Sacubitril/valsartan is a conjugation molecule that combines valsartan, an angiotensin receptor blocker, with sacubitril, a neprilysin inhibitor. Since the first investigational experience was done in the PARADIGM-HF study [1], this drug has fueled the hopes and enthusiasms of many doctors and patients due to the fact that at the target dose of 400 mg, it was shown to be more effective than enalapril given at the dose of 20 mg per day regarding the clinical endpoints of mortality and heart failure hospitalization. Thanks to the huge amount of favorable findings, one only trial, i.e. the PARADIGM-HF, was sufficient to convincingly demonstrate the efficacy of this molecule (rating IA). Therefore, sacubitril/valsartan triumphantly entered the armory of evidence-based drugs for heart failure with reduced left ventricular ejection fraction (HFREF).
While a clinical amelioration has been demonstrated with certainty, namely less deaths, less heart failure hospitalizations, etc., it is not shown with with equal clarity which improvements in echocardiographic measures of reverse remodeling are induced by this drug so as to accompany and justify such a brilliant clinical amelioration [2]. In fact, the clinical efficacy appears to be higher than one would expect based on the drug-induced variations of left ventricular ejection fraction (LVEF). Regarding this parameter, some have documented an only mild increase in the short term in patients treated with sacubitril/valsartan compared to controls [3]. On the contrary, other researchers have demonstrated an obvious increase in LVEF following a median of 11 (25-75th percentile; 9 - 13) months of treatment [4]. However, the introduction into the clinical practice of speckle tracking echocardiography (STE) [5-7] has made it possible to shed light on another very important determinant of ventricular pump efficiency, namely the left ventricular systolic deformation in the cranio-caudal direction, i.e. the so-called global longitudinal strain (GLS). This index does not overlap, in terms of the importance and quality of the information provided, the E/e’ ratio [8] that is the parameter inferable from the integrated use of conventional echocardiography and tissue Doppler imaging. In fact, GLS is presented not as an index of diastolic function but as a measure of the efficiency of systolic contraction along the longitudinal axis of the left ventricle [8]. The GLS implicitly represents a criticism of the concept that the insufficiency of left ventricular diastolic relaxation, attributed to about 50% of cases of chronic heart failure, i.e. patients with preserved ejection fraction (HFpEF) [9], plays the main role as a causative factor for the development of HFpEF. Actually, in our opinion, it is very likely that HFpEF does not arise from the poor relaxation capacity of the ventricular wall during the diastole, but rather from a defective performance of the longitudinal fibers that are involved in the systolic basis-apex deformation of the left ventricle. The complex chapter of the HFpEF phenotypes could be partially rewritten putting in the right light the importance of the basis-apex deformation of the left ventricle. This deformation contributes to the realization of an adequate stroke volume and occurs during systole, simultaneously with the deformation along the transverse direction, the latter measured by the LVEF.
| Materials and Methods | ▴Top |
In our retrospective cohort study, we separated patients treated with sacubitril/valsartan from those treated with conventional medical therapy, including angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers (ARBs). For the rest, the therapies practiced in the two groups, patients under sacubitril/valsartan and controls, were almost identical, including similar doses of beta-blockers and mineralocorticoid receptor antagonists (MRAs) in the two cohorts, plus loop diuretic, furosemide or torsemide, administered at variable doses depending on the intensity of dyspnea and edema severity. The Institutional Review Board Approval was not required, considering the study features (retrospective cohort study). Moreover, this study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration. This study did not involve experiments on animals.
Thanks to a careful study of the medical records, the precise moment of the introduction in therapy of the sacubitril/valsartan was noted, and the time of exposure to the sacubitril/valsartan was calculated for each patient retrospectively enrolled. Both in the treated patients and in the controls, the GLS values detected at the beginning of sacubitril/valsartan therapy or during conventional treatment, respectively, and those measured after not less than 1 year, both during sacubitril/valsartan and conventional treatment, were recorded.
The data collected from the medical records of two different hospitals (“Casa Sollievo della Sofferenza” Hospital and S. Maria del Pozzo Clinic) were statistically processed. In particular, the controls and the treated patients were initially recruited retrospectively like a casual consecutive series. Subsequently, according to the propensity score matching method [10], controls and patients with basal clinical characteristics as similar as possible were gathered in a 2:1 ratio. In this regard, the basal characteristics of patients and of their matched controls are reported in Table 1. The data were extracted from medical records which dated back to the years 2017 and 2018. More exactly, the retrospective observation covered the time span between January 1, 2017 and December 31, 2018.
 Click to view | Table 1. Comparison of Demographics and Clinical, Laboratory and Echocardiographic Features of Patients Examined in the Retrospective Study According to Whether or Not a CHF Patient Was Treated With Sacubitril/Valsartan |
Importantly, the authors of the present retrospective cohort study did not have any decisional role in the therapies, but they merely accomplished the task of acquiring and subsequently processing the data for scientific research. The doctors who had prescribed and implemented the therapies did not participate in the statistical processing of the data. Likewise, they had no role in the writing of the present article. Furthermore, it was not consistently possible to identify a rational criterion, capable of systematically justifying the indication of the doctors to use sacubitril/valsartan therapy or, alternatively, to prefer conventional therapy. In fact, the reason for the switch from therapy with ACE inhibitors or ARBs to that with sacubitril/valsartan was usually not specified in the clinical sheets.
All patients, for whom a telephone number was available, were asked to explicitly declare their will to grant the use of their clinical data for purposes of scientific research after being informed of the aims of the study and of its compliance with rigorous criteria of preservation of anonymity and protection of individual privacy. A general consent was recorded, expressed via phone, to the concession of their personal data, provided that they were aggregated and processed in an anonymous way.
Echocardiography
The evaluation of the echocardiograms was accomplished by means of a Vivid 7 (General Electric, Horten, Norway) echocardiographic machinery. A frame rate of 60 - 75/s was used for acquiring the images. Then, they were digitally transferred to a remote workstation for offline analysis (Echopac BT 11.1.0, General Electric, Horten, Norway). All analyses were performed by only one experienced operator who had been kept blinded to clinical and biochemical data concerning both the patients, i.e. subjects taking sacubitril/valsartan, and controls. Two-dimensional speckle tracking echocardiography was carried out using a semiautomatic algorithm.
In brief, using manual determination, three reference points (two annular and one apical) were chosen in each of the three apical views, so as to enable the software to monitor the myocardium in a semi-automated manner during the entire course of the cardiac cycle. Each ventricular wall was then splitted into three segments so as to achieve the generation of 17 segments encompassing the entire myocardium. Thorough manual inspection for tracking purposes was carried out, and in the case of imperfect tracking, the segment was removed from the analysis. Longitudinal strain curves were built for each segment and the maximum value was calculated. The GLS was then inferred as the mean of all 17 segments.
Statistical analysis
All statistical tests were performed with a commercially available statistical analysis program (SPSS 15.0 for Windows, SPSS Inc., Chicago, IL, USA). The distribution of the data was assessed using the one-sample D’Agostino-Pearson test. Continuous variables displaying normal distribution were expressed as mean ± standard deviation (SD). If highly skewed, however, continuous variables were presented as medians with interquartile ranges (25-75th percentile). Categorical variables were presented as %. To reduce the risk of bias resulting from different patient characteristics in both groups, the final analysis population was defined based on propensity score-matched (PSM) cohorts. We applied a logistic regression model. Several variables were found to be significantly associated with the probability of belonging to one of the groups, based on a backward stepwise elimination (P = 0.05 cut-off) methodology. The following variables were finally used to calculate the propensity score for each patient: age and care level at index date, anticoagulant use, antianginal drug use, insulin use, occurrence of stroke and hospitalization costs in the baseline period. Patients were matched 2:1 within gender-specific 5 years age groups, based on their propensity score with a maximum allowable difference of 0.001. To examine the changes of parameters before and after treatments (intragroup comparison), the paired samples t-test or the Wilcoxon signed-rank test were applied. Chi-square test was used for comparisons concerning categorical variables.
| Results | ▴Top |
One hundred thirty-two patients were collected within our retrospective cohort study, of whom 44 were treated with sacubitril/valsartan and 88 were subjected to conventional therapy. All patients had HFREF. The basal characteristics of patients are reported in Table 1. The mean duration of the period spent from the first to second detection of echocardiographic parameters, i.e. LVEF and GLS, was 14 ± 3 months. In the group of patients treated with sacubitril/valsartan, LVEF and LV GLS findings were obtained either basally, i.e. before the shift to sacubitril/valsartan therapy, or after at least 1 year of therapy with the new agent. In the control group, both LVEF and LV GLS measurements were calculated during conventional therapeutic regimen. Furthermore, also in the group of controls, in analogy with that of the sacubitril/valsartan-treated patients, both for the LVEF and the LV GLS, it was decided to consider echocardiographic measurements separated from one another by a time interval of at least 1 year.
In the controls, LVEF was improved after 1 year of therapy from 38.071 ± 5.445% (mean ± SD) to 41.595 ± 5.282% (P = 0.003) (Fig. 1). Instead, no significant improvement in the controls could be identified for the LV GLS by comparing two consecutive measurements separated by a time span of 1 year from -12.059 ± 4.016% (mean ± SD) to -12.250 ± 4.287% (P = 0.406) (Fig. 2).
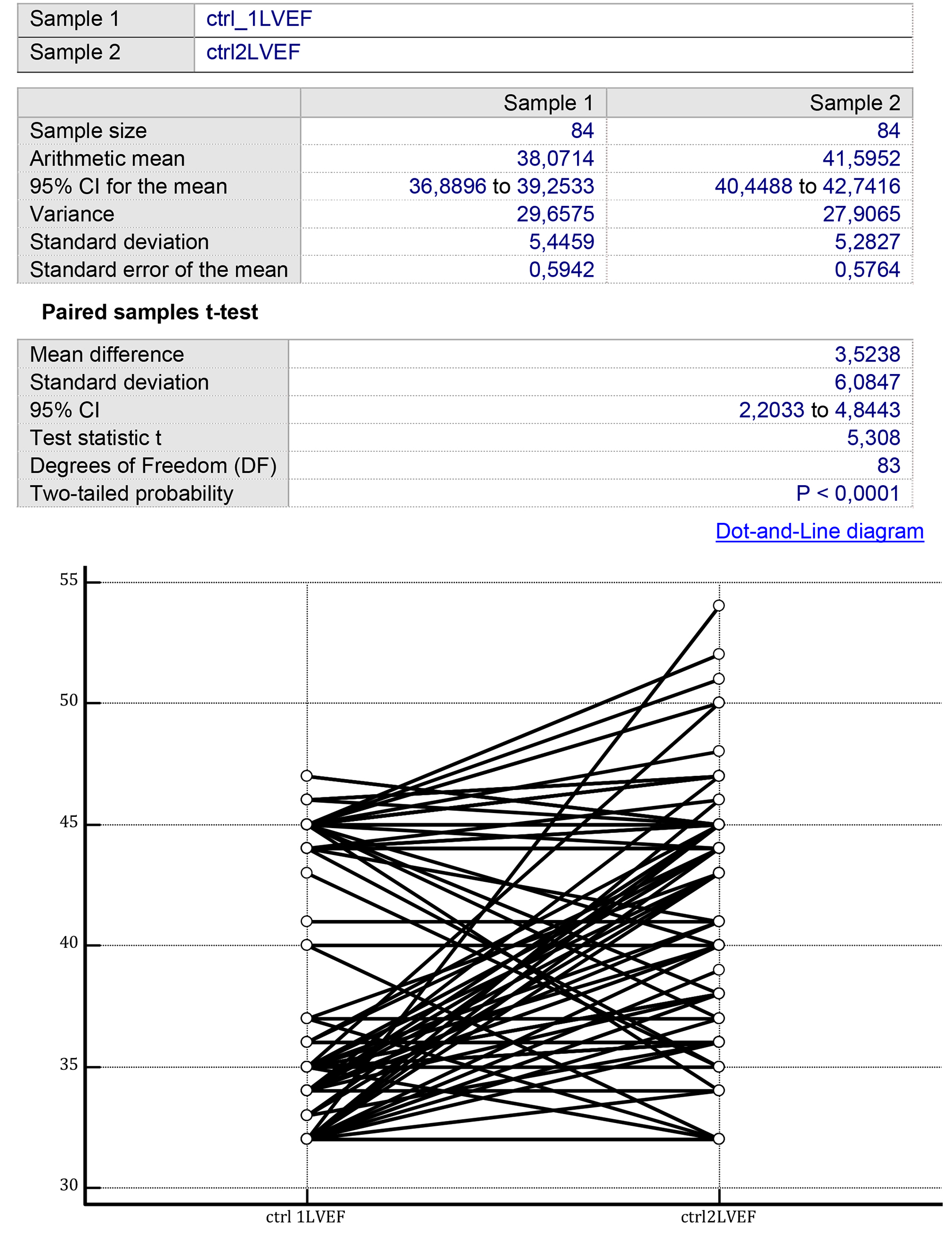 Click for large image | Figure 1. On the two sides of the figure, there are the LVEF values collected from the group of CHF patients treated with conventional therapy over a mean therapy duration of 14 ± 3 months. Initial mean LVEF value: 38.07 ± 5.44%; final mean LVEF value: 41.59 ± 5.28% (P < 0.0001) (paired samples t-test). LVEF: left ventricular ejection fraction; CHF: chronic heart failure. |
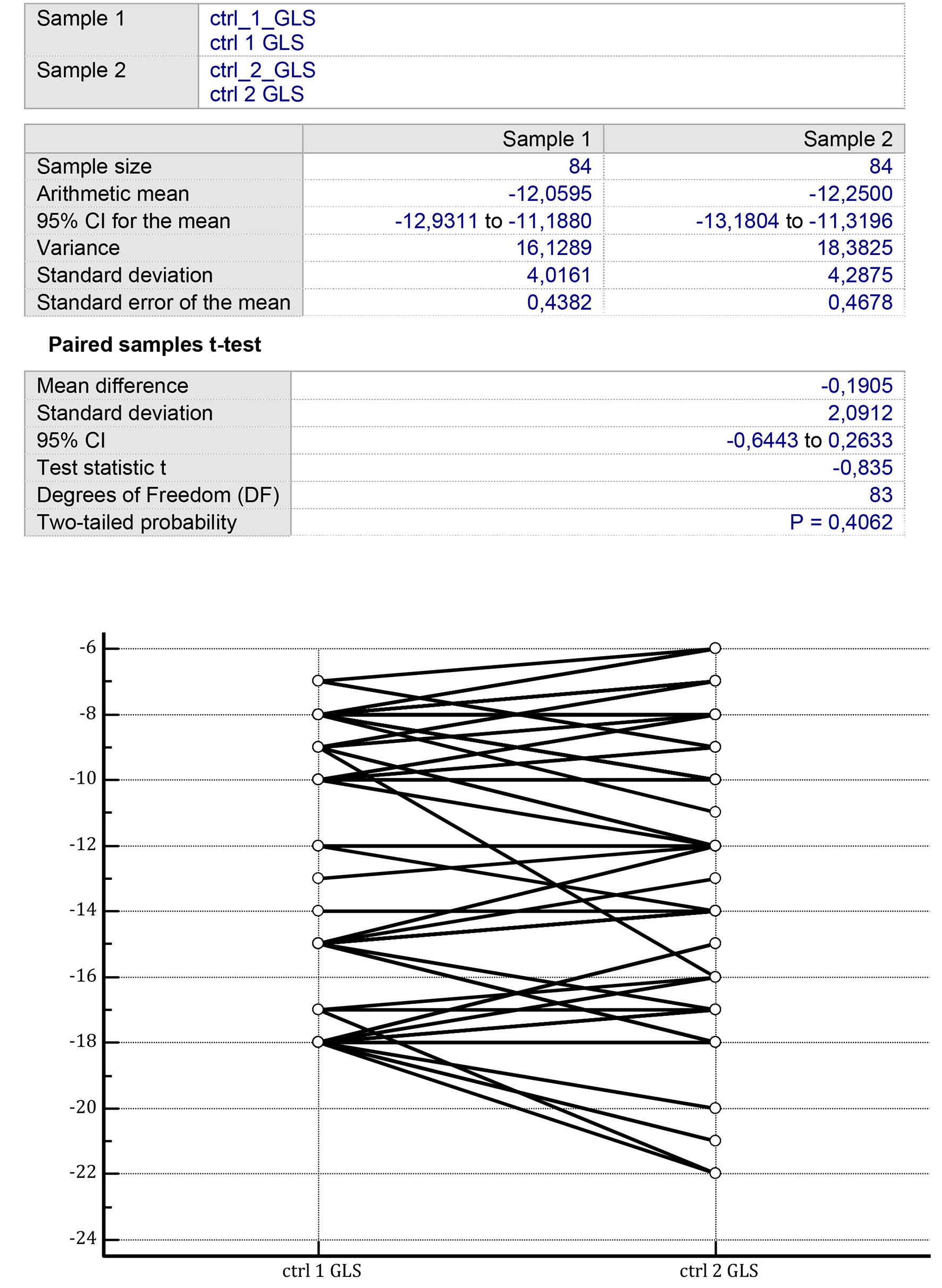 Click for large image | Figure 2. On the two sides of the figure, there are the GLS values collected from the group of CHF patients treated with conventional therapy over a mean therapy duration of 14 ± 3 months. Initial mean GLS value: -12.05 ± 4.01%; final mean GLS value: -12.25 ± 4.28% (P = 0.40) (paired samples t-test). GLS: left ventricular ejection fraction; CHF: chronic heart failure. |
In analogy with controls, patients assigned to sacubitril/valsartan showed a significant increase in LVEF after 1 year of treatment from 39.714 ± 4.789% (mean ± SD) to 42.119 ± 5.683% (P < 0.001) (Fig. 3). However, differently from the controls, the sacubitril/valsartan group exhibited a significant improvement in LV GLS in the measurements performed after 1 year from -10.142 ± 3.080% to -18.238 ± 7.284% (P < 0.001) (Fig. 4).
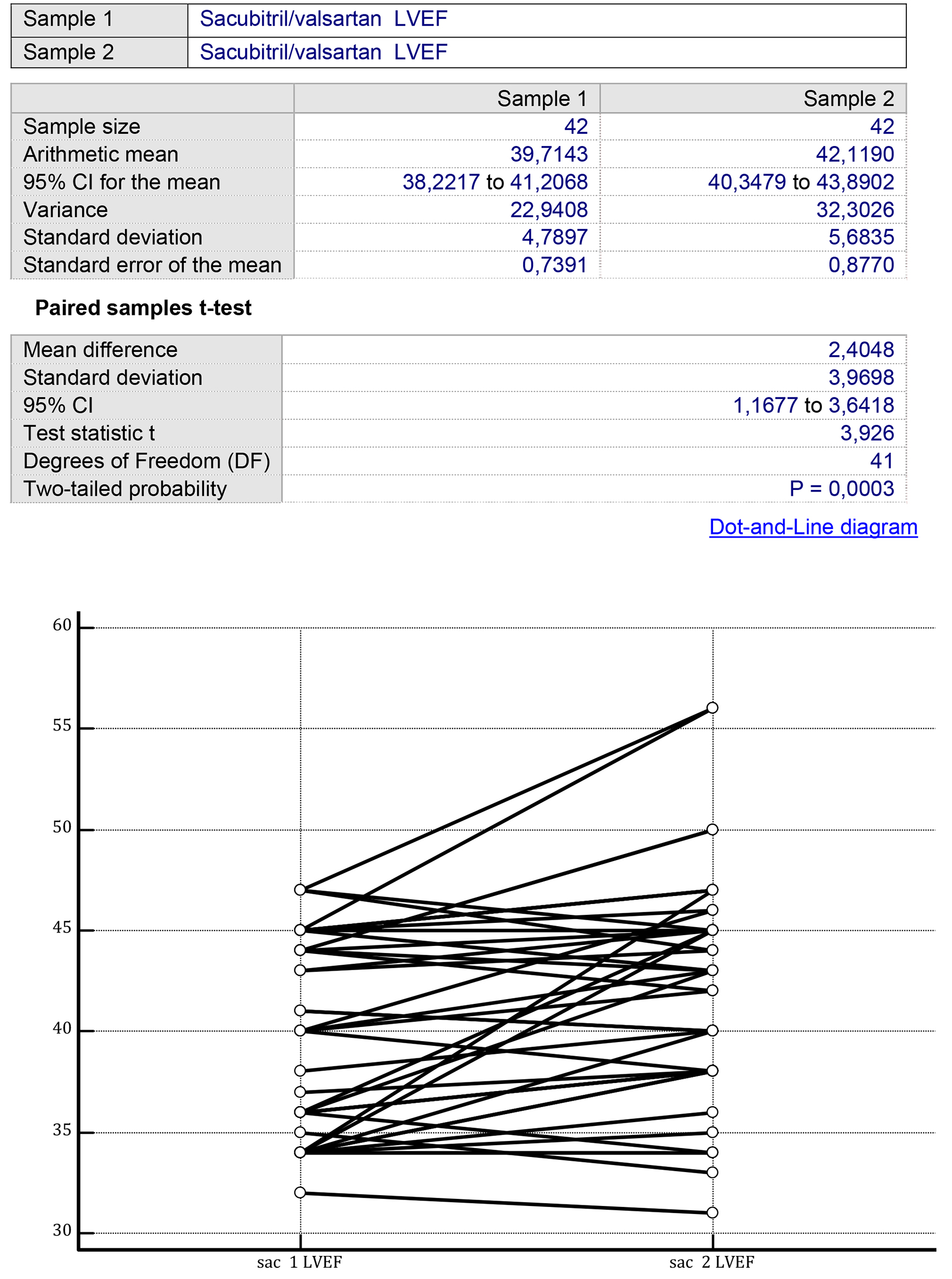 Click for large image | Figure 3. On the two sides of the figure, there are the LVEF values, recorded before the onset of the therapy with sacubitril/valsartan (left side) and after a mean therapy duration of 14 ± 3 months (right side). Initial mean LVEF value: 39.71 ± 4.78%; final mean LVEF value: 42.11 ± 5.68% (P = 0.0003) (paired samples t-test). LVEF: left ventricular ejection fraction. |
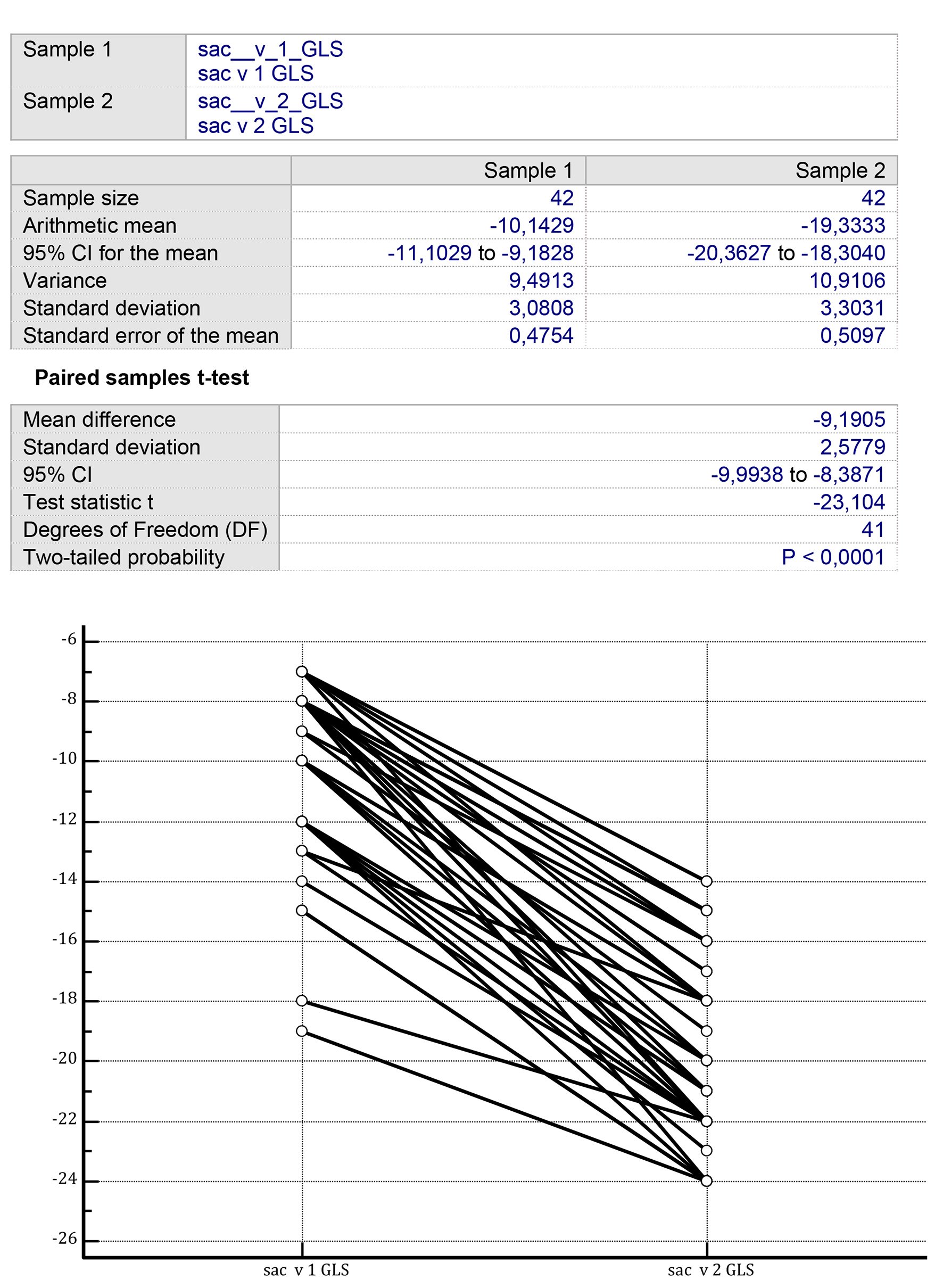 Click for large image | Figure 4. On the two sides of the figure, there are the GLS values, recorded before the onset of the therapy with sacubitril/valsartan (left side) and after a mean therapy duration of 14 ± 3 months (right side). Initial mean GLS value: -10.14 ± 3.08%; final mean GLS value: -18.23 ± 7.28% (P < 0.001) (paired samples t-test). GLS: global longitudinal strain. |
| Discussion | ▴Top |
Our study population included only cases of HFREF. Notably, an impaired longitudinal strain is able to considerably contribute to the depression of stroke-volume and cardiac index, determining the occurrence of signs and symptoms of heart failure. Actually, in the last period, after the introduction into the current use of STE, the concept of the left systolic ventricular dynamics has changed, by admitting that it consists of two fundamental components, the shortening along the transverse axis and that along the longitudinal axis. The first is expressed by the LVEF, while the second is quantified by the determination of the LV GLS. A discrepancy may occur, namely the normality of an index is in contrast with the obvious impairment of the other. This phenomenon is typically represented in the HFpEF, in which an impaired LV GLS coexists with a normal LVEF. Instead, in HFREF patients, it is typical to find an alteration involving simultaneously, even if often with different intensity, both the transverse (radial) function expressed by the LVEF and the longitudinal function represented by the LV GLS.
Prior to the introduction of STE, the measurement of possible favorable effects of a pharmacological therapy on the ventricular remodeling in decompensated patients with dilated left ventricle was based exclusively on the assessment of the evolution of LVEF over time. In particular, a possible therapeutic effect consisting in an LVEF increase was sought in order to ascertain that the drug played a role as a protective agent, by propitiating a favorable remodeling of the geometry of the left ventricular chamber. In this way, with the use of periodic determinations of LVEF, it was possible to highlight that drugs such as ACE inhibitors, beta-blockers or MRAs cause an improvement of left ventricular parietal kinetics. In fact, for each of these classes of drugs, an increase in the LVEF in the medium-long term has been highlighted. This was the echocardiographic equivalent of the improvements in the “hard” clinical outcomes observed with these drugs, e.g. all-cause mortality and hospitalization due to heart failure.
In patients treated with sacubitril/valsartan, the innovative mechanism of action, i.e. the enhancement of the effect, consisting in reduction of wall stress exerted by the atrial natriuretic peptide (ANP) and by the B-type natriuretic peptide (BNP), because of inhibition of their enzymatic degradation, has translated into a reduction in mortality from all causes, heart failure hospitalizations and major adverse cardiovascular events [1]. However, the echocardiographic equivalent of these very brilliant clinical outcomes has not been completely clarified yet.
In fact, the increase in the LVEF, as reported for sacubitril/valsartan, is no greater than that found with the use of enalapril [3]. More in-depth investigations with the use of indicators of longitudinal systolic function have been therefore recommended to verify whether a part of the clinical improvement could be supported by a reverse remodeling not resulting only in an LVEF increase. Really, the intervention of a favorable effect of sacubitril/valsartan not only on the transverse parietal kinetics but also on the longitudinal shortening of the fibers, has been confirmed by our retrospective cohort study.
Indeed, the study showed that the drug in the long term (mean duration of retrospective observation: 12 months) is characterized by the fact of acting in a balanced manner on the global systolic function, the latter resulting from the integration of the transverse contraction with the basis-apex contraction. In fact, in partial contrast with patients taking ACE inhibitor or ARBs, it was found that the effect of sacubitril/valsartan involves both components of the systolic parietal kinetics, but seems to be more pronounced at the level of the base-to apex contraction of the left ventricle (LV GLS measurements after 1 year from -10.142 ± 3.080% to -18.238 ± 7.284%; P < 0.001).
Our findings are important, even if they arise from an observational study and are therefore more prone to biases. In fact the results of the present study pave the way to insightful hypotheses of possible use of the drug in the conditions of selective or preferential damage to the GLS, i.e. in patients with HFpEF. In fact, the impairment of GLS has emerged in the last period as a pathognomonic trait of the majority of HFpEF phenotypes, even in the cases where the indicators of diastolic function (E/e' and e' velocity) appear to be within the limits of the norm [8]. Furthermore, HFpEF, more than by a deficit of diastolic function, which is an inconstant finding [9] would be characterized by an almost systematic weakening of the systolic longitudinal contraction of the subendocardial fibers, implying a poor base-to apex systolic deformation of the left ventricle.
In addition, in some common cardiac diseases, such as hypertensive, diabetic or hypertensive-diabetic heart disease, longitudinal systolic dysfunction would have a prominent role in the genesis of heart failure, that is, it would be the primum movens of HFpEF, regardless of the possible co-existence of defective diastolic compliance (E/e' ratio ≥ 15).
Furthermore, in our retrospective study, the rigidity-hypokinesia along the base-to apex direction of the left ventricle, mirrored by a reduced GLS, was effectively corrected by the administration of sacubitril/valsartan, but not by conventional therapy with ACE inhibitor or ARBs.
Hence, it has been hypothesized that sacubitril/valsartan might be indicated also for the HFpEF, which is precisely characterized by selective GLS depression, with LVEF within the limits of the norm. However, this is only a hypothesis that springs from a retrospective investigation. It is hoped that ongoing randomized controlled trials (RCTs) will provide more complete and convincing answers in this regard.
Conclusions
The present retrospective cohort study demonstrates that the use of sacubitril/valsartan for HFREF patients, extended for a mean duration of 1 year, yields a significant improvement in the echocardiographic parameters of transverse (LVEF) and sagittal (LV GLS) systolic function. For the latter in particular, a clear superiority emerges in comparison with conventional therapy including ACE inhibitor or ARBs. From these data, the hypothesis could be derived of a possible useful role of the sacubitril/valsartan also for the therapy of HFpEF. In this regard, more exhaustive clarifications ensuing from the ongoing RCTs are eagerly awaited.
Acknowledgments
None.
Financial Disclosure
The authors Renato De Vecchis, Andrea Paccone and Marco Di Maio declare that the present article has not benefitted from any source of funding.
Conflict of Interest
The authors Renato De Vecchis, Andrea Paccone and Marco Di Maio do not have any conflict of interest to declare concerning the present article.
Informed Consent
Not applicable.
Author Contributions
RDV and AP contributed to conceptualization; RDV contributed to data curation; RDV, AP and MDM contributed to writing and original draft preparation; RDV, AP and MDM contributed to writing, review and editing.
| References | ▴Top |
- McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, Rouleau JL, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
doi pubmed - Almufleh A, Marbach J, Chih S, Stadnick E, Davies R, Liu P, Mielniczuk L. Ejection fraction improvement and reverse remodeling achieved with Sacubitril/Valsartan in heart failure with reduced ejection fraction patients. Am J Cardiovasc Dis. 2017;7(6):108-113.
- De Vecchis R, Ariano C, Di Biase G, Noutsias M. Sacubitril/valsartan for heart failure with reduced left ventricular ejection fraction : A retrospective cohort study. Herz. 2019;44(5):425-432.
doi pubmed - Santangelo G, Bursi F, Toriello F, Valli F, Tombolini E, Torta D, Bosotti L, et al. Sacubitril/valsartan improves medium-term reverse left ventricular remodeling: why wait? J Cardiovasc Med (Hagerstown). 2019.
doi pubmed - Geyer H, Caracciolo G, Abe H, Wilansky S, Carerj S, Gentile F, Nesser HJ, et al. Assessment of myocardial mechanics using speckle tracking echocardiography: fundamentals and clinical applications. J Am Soc Echocardiogr. 2010;23(4):351-369; quiz 453-355.
doi pubmed - Shah AM, Claggett B, Sweitzer NK, Shah SJ, Anand IS, Liu L, Pitt B, et al. Prognostic Importance of Impaired Systolic Function in Heart Failure With Preserved Ejection Fraction and the Impact of Spironolactone. Circulation. 2015;132(5):402-414.
doi pubmed - Tadic M, Pieske-Kraigher E, Cuspidi C, Genger M, Morris DA, Zhang K, Walther NA, et al. Left ventricular strain and twisting in heart failure with preserved ejection fraction: an updated review. Heart Fail Rev. 2017;22(3):371-379.
doi pubmed - Kraigher-Krainer E, Shah AM, Gupta DK, Santos A, Claggett B, Pieske B, Zile MR, et al. Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. J Am Coll Cardiol. 2014;63(5):447-456.
doi pubmed - Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539-2550.
doi pubmed - Grotta A, Bellocco R. A review of propensity score: principles, methods and application in Stata. Italian Stata Users Group Meeting - Milan, 13 November 2014; p. 24-45.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.