

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 2, April 2022, pages 97-103

Ablation Index Outcome in Redo Persistent Atrial Fibrillation Ablation: Results of a Short-Term Study
Sarah Jane Lennona, James Manniona, Edward Keelana, Jim O’Briena, Gael Jauverta, Enes Elvin Gulb, Usama Bolesa, c
aHeart and Vascular Centre, Cardiology Department, Atrial Fibrillation Institute, Mater Private Hospital, Dublin, Ireland
bMadinah Cardiac Center, Arrhythmia Service, Madinah, KSA
cCorresponding Author: Usama Boles, Heart and Vascular Centre, Atrial Fibrillation Institute, Cardiovascular Research Institute (CVRI), Mater Private Hospital, Dublin 7, Ireland; Usama.boles@materprivate.ie
Manuscript submitted November 28, 2021, accepted January 14, 2022, published online April 5, 2022
Short title: AI Outcome in Redo peAF Ablation
doi: https://doi.org/10.14740/cr1337
| Abstract | ▴Top |
Background: Ablation index (AI) is a novel catheter-based parameter that has improved the outcome and safety of radiofrequency (RF) ablation of pulmonary vein isolations (PVIs). This index incorporates contact force (CF) (g), time (s), and power (W) parameters. The role of AI in redo ablations for persistent atrial fibrillation (peAF) has not been fully investigated. Hence, the impact of AI on the success of the redo PVI during the short-term follow-up period is the aim of this study.
Methods: A retrospective analysis of 39 consecutive patients who underwent redo PVI ablations for peAF was carried out between January 2016 and December 2018. Target values for AI were 500 - 550 for anterior and roof and 400 - 380 for posterior and inferior regions. We compared outcomes between AI-guided and catheter CF ablations (i.e., forced time integral (FTI) of more than 400 g/s) during a follow-up of 24 months.
Results: Pulmonary vein reconnections at redo procedure were similar in both groups (P = 0.1). AF free burden period was non-significant (mean 15.53 ± 2.4 months in AI group vs. 15.22 ± 1.9 months in CF group, P = 0.79) at 24 months. The AI group demonstrated greater numbers of patients for whom anti-arrhythmic therapy could be de-escalated over 1 year (n = 11 (65%) in AI vs. n = 6 (27%) in CF, P = 0.02). Fewer patients underwent escalation of their anti-arrhythmic therapy (n = 2 (12%) in AI vs. n = 7 (32%) in CF, P = 0.15). The AI group trended towards a shorter procedure time (111.6 ± 27 min) compared to the CF group (133 ± 40 min) (P = 0.06). Other procedural details were comparable.
Conclusion: Redo PVI interventions using AI lead to a significant de-escalation in medication during follow-up. Procedure time and radiation dose using AI tends to be shorter. Both techniques are safe with minimal complications.
Keywords: Pulmonary vein isolation; Persistent AF; Ablation index; Contact force
| Introduction | ▴Top |
Pulmonary vein isolation (PVI) has been well established as an effective method for the maintenance of sinus rhythm (SR) in atrial fibrillation (AF) management [1]. The technique has shown greater success in the treatment of paroxysmal AF (PAF) in comparison to persistent AF (peAF) as the recurrence rate remains high in peAF, leading to redo procedures [2-5].
The common etiology of the recurrence is often related to reconnections of the wide antral circumferential ablation (WACA) lines of the pulmonary veins 6]. EFFICAS I and II studies optimized lesion size and improved efficacy for PVI procedures [7, 8]. Despite advances and optimization of catheter parameters including tissue contact force (CF) and force time integral (FTI), ablation power was not previously taken into account [6, 9]. Ablation index (AI) is a novel parameter which incorporates CF, time, and power in deliverance of ablation lines [10, 11]. It has been shown to produce more durable outcomes in comparison to the CF catheter technique alone using the equation for AI (CF (g), time (s), and power (W) parameters) [2, 12]. The equation of AI is calculated as follows: AI = [11]. AI has the potential to optimize results of PVI as well as minimize procedure-related complications, and improved procedure details (i.e., radiation exposure, fluoroscopy time and procedure time) [2]. Due to these benefits, AI utilization has been adapted widely as the primary modality of PVI execution [11, 12].
We propose the comparison of the outcomes of redo AI-guided ablation for peAF to the previously widely used catheter-enabled CF ablation/FTI target of 400 m/s.
| Materials and Methods | ▴Top |
We carried out a single-center retrospective study (Mater Private Hospital, Dublin) in which 39 consecutive patients with peAF were included. Group 1 included patients who underwent redo CF procedures, from January 2016 until March 2017. Group 2 included patients who underwent redo AI procedures, from July 2017 until August 2018. All follow-up data were from 2 years post redo procedure. Definitions of persistent and follow-up monitoring were based on the American College of Cardiology [13]. Each operator conducted a high volume of procedures, a minimum of 100 ablations each per year. Approved institutional review board reference is 1/378/2218 TMR. This study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declarations.
Inclusion criteria
There were several parameters set to homogenize the data. All patients must have had one prior PVI to be included. Patients had de novo peAF, and those who had paroxysmal or other atrial tachycardias were excluded. All patients were above 18 years of age. Prior anti-arrhythmic therapy was not an inclusion factor (Supplementary Material 1, www.cardiologyres.org).
Procedure details
Patients underwent general anesthesia, and venipuncture was performed in the right femoral vein to allow for vascular access. The presence of left atrial appendage (LAA) thrombus was excluded by trans-esophageal echocardiography (Vivid S70N, GE Healthcare, USA). The latter also guided the transeptal puncture where 7-Fr mapping catheters were introduced into left atrium (LA) for mapping (each with 20 electrodes; LASSO, Biosense-Webster, Inc., Belgium). The mapping catheter generated a 3D fast-anatomical map (FAM) with widely used reconstruction software (CARTO3 CONFIDENSE Mapping Module, Biosense-Webster, Inc., Belgium). All patients received unfractionated heparin according to body weight and maintaining activated clotting time (ACT) 250 - 300 s.
Ablation strategies
The pulmonary veins were first re-isolated as standard with a WACA line or ablating any identified reconnections in previously created lines. Additional lines were also added as required as per the operating electrophysiologists’ clinical judgement. Additional ablation lines occurred in such areas as the posterior wall, roof, cavo-tricuspid isthmus, and mitral isthmus.
AI and CF
The AI parameters for group 1 (AI group) were set as 400 - 550 for the anterior wall and 380 - 400 for the posterior and inferior regions. For contact force only patients in group 2 (FTI group), redo PVI was carried out using the original CF catheter technique (FIT).
Patient follow-up
Patients were followed up for 24 months post-procedure. Heart rhythm was assessed using electrocardiography (ECG), Holter or through cardiac implanted electronic device. Data collected from all available patients’ records as AF recurrence (i.e. from clinic letters, electrical synchronized cardioversion post ablation, allied health care reports and remote ECG monitoring). A 3-month blanking period was applied, and the data were not censured from the outcome during this time. The patient’s anti-arrhythmic drugs (AADs) were recorded from post-procedure up to 6 months, recording any change and/or dosage alterations in AADs. This was documented as a de-escalation of therapy, measured as the reduction in number of AADs, or a reduction in dose. Conversely, escalations or no change were also recorded.
Statistical analysis
Statistical analysis was carried out using IBM SPSS Statistic Version 26 (IBM®). Kaplan-Meier graphs were used to evaluate the AF free interval over the follow-up period. Significance between outcomes was performed by log rank analysis. All continuous variables were expressed as the mean and standard deviation. The Student’s t-test was used for unpaired group comparisons. All tests were two-sided, with a P < 0.05 indicating statistical significance.
| Results | ▴Top |
Patient characteristics
The demographics and characteristics of AI group and CF group are shown in Table 1. There was no significant difference between group demographics. There were no intra-procedural complications and no post-procedure complications in either patient group (Table 2). Procedure details were similar in both groups regarding radiation dosage and fluoroscopy time within this patient cohort (Table 1). The mean procedure time was shorter in the AI group but did not reach significance (P = 0.055).
 Click to view | Table 1. Summary of Patient Demographics, Anti-Arrhythmic Drugs and Procedure Details |
Click to view | Table 2. Summary of Follow-Up, Outcomes and Complications |
AI vs. CF success to maintain SR
There were 21 episodes of AF recorded across both cohorts, once recorded the patient’s remaining data were censored, outside of the blanking period. In the AI group, nine patients (53%) were in SR at 1 year compared to 13 patients (59%) in the CF group. The mean AF free interval was 9.35 ± 1 months in the AI group vs. 9.68 ± 0.86 months in CF group (Fig. 1). There was no significant difference between both groups on free AF time at 1 year (P = 0.9).
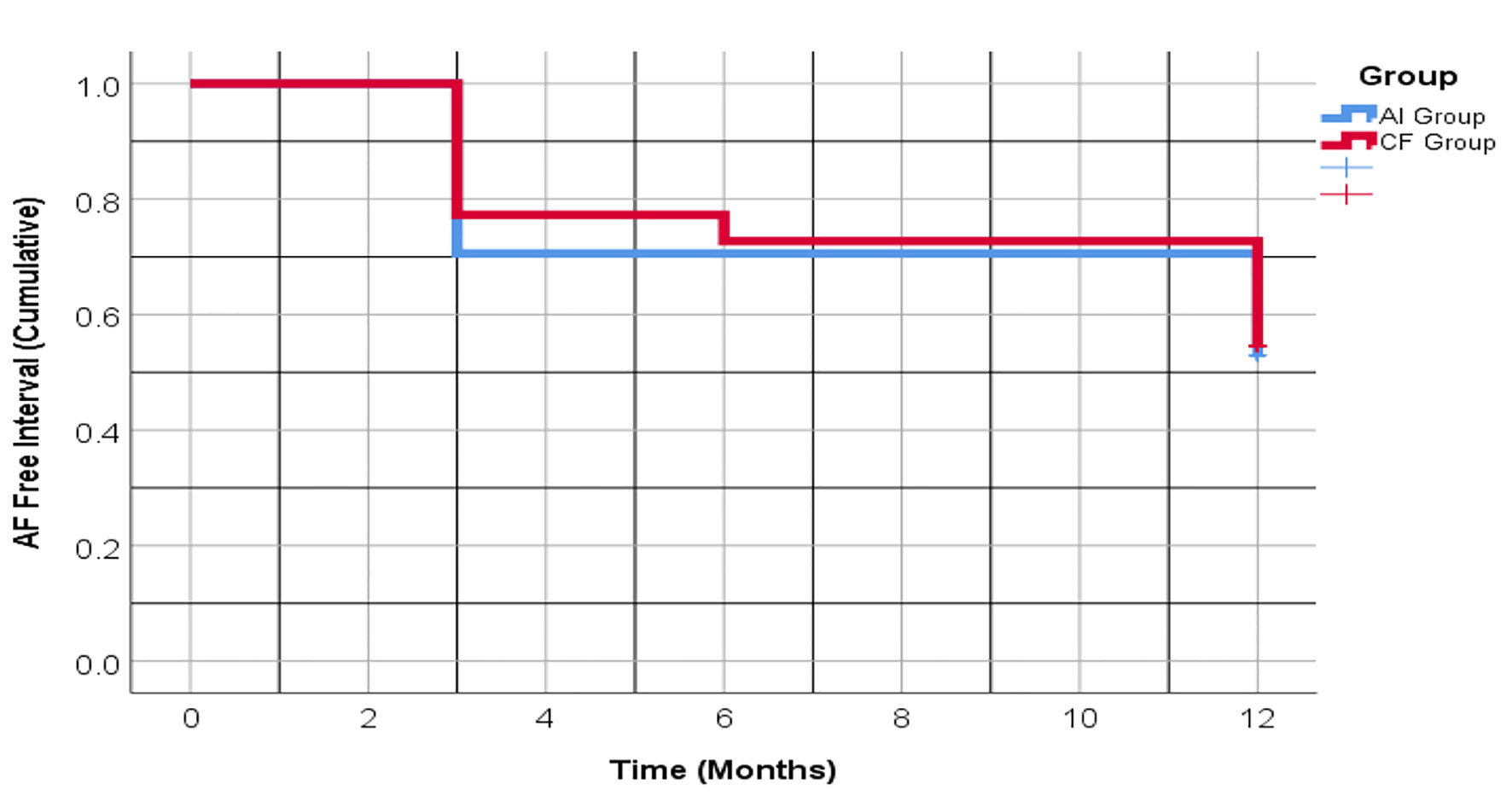 Click for large image | Figure 1. Kaplan-Meier analysis of AF recurrence at 12 months between the AI and CF groups, following redo PVI procedure, with adjusted 3-month blanking period. Y-axis demonstrates cumulative data for each group. Once AF was detected, the patient’s data were censored from follow-up. Blue line represents the AI interventional group. Red line represents the CF group. AF: atrial fibrillation; AI: ablation index; CF: contact force; PVI: pulmonary vein isolation. |
The Kaplan-Meier chart in Figure 2 shows the AF free interval at 2 years. There was no significant difference in outcomes between the AI and CF groups (P = 0.79) after 24 months (Fig. 2). The mean AF free interval for the AI group was 15.53 ± 2.4 months, in comparison the mean AF free interval for the CF group was 15.22 ± 1.9 months. There were seven patients without full follow-up data up to 24 months in the AI group, and five patients in the CF group. The data were censored on last date of follow-up period.
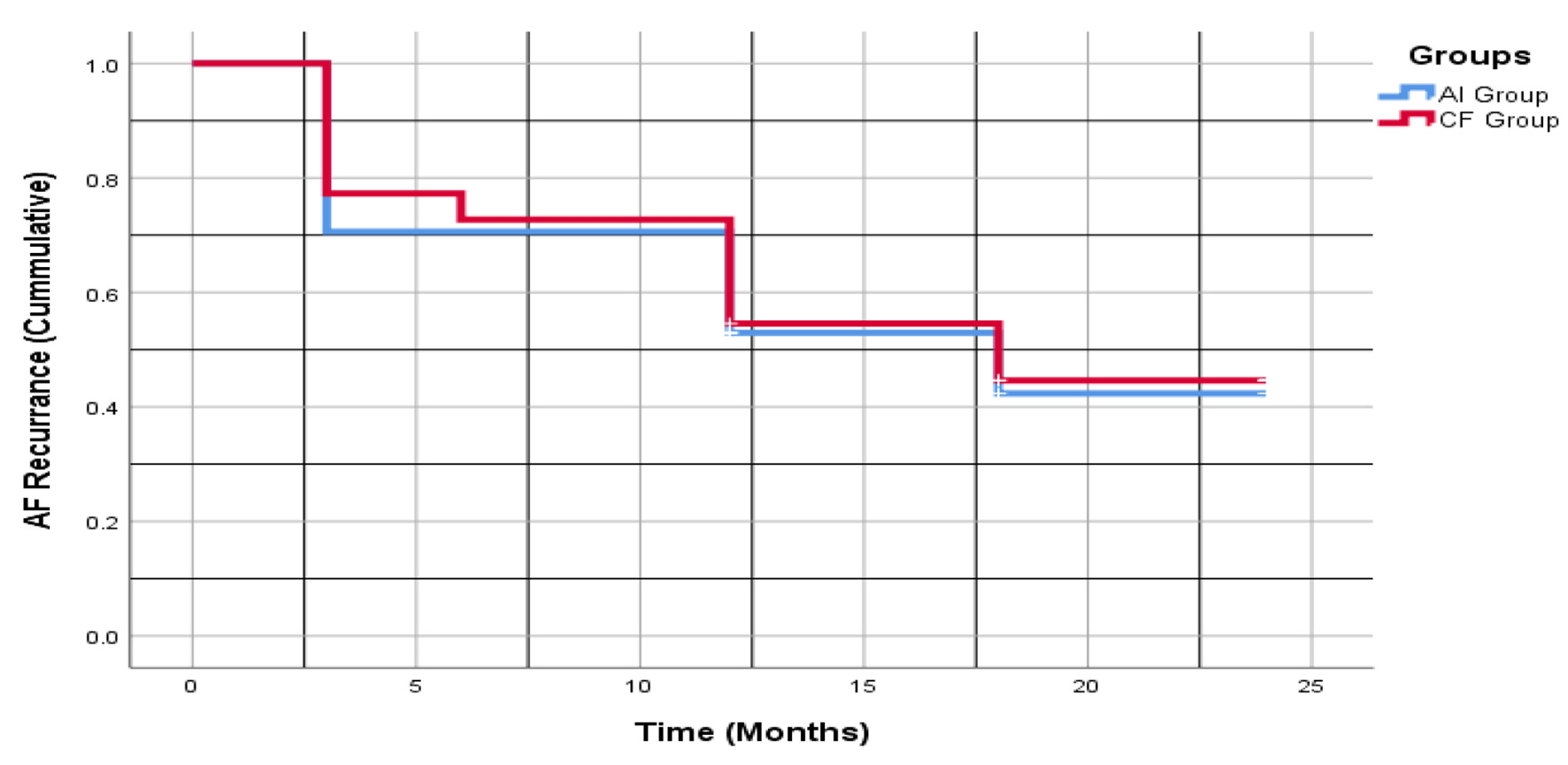 Click for large image | Figure 2. Kaplan-Meier analysis of AF recurrence at 24 months between the AI and CF groups, following redo PVI procedure, with adjusted 3-month blanking period. Blue line represents the AI interventional group. Red line represents the CF group. AF: atrial fibrillation; AI: ablation index; CF: contact force; PVI: pulmonary vein isolation. |
Early recurrence during the blanking period
There were six episodes (27%) of early AF recurrence at 6 weeks in the CF group, four of which required direct current cardioversions (DCCVs). There were three episodes of early recurrence at 6 weeks in AI group (18%), all requiring DCCVs. All patients with early detected recurrence proceeded to have AF detected again after the blanking period. The rate of early recurrence was not significantly different between the CF and AI groups before the blanking period (P = 0.49).
Ablation lines and the impact on maintenance of SR
Additional lines were created in most patients that presented for redo PVI in both patient cohorts (Table 1). There was a significantly greater incidence of additional ablation line created at redo ablation in the AI group. There were 14 patients (83%) in the AI group compared to 14 patients in the CF group (64%) (P = 0.01). When a subgroup analysis of the cohorts that had PVI with additional lines was carried out between groups, it showed no significant difference on the outcome, i.e., maintaining SR (P = 0.7).
Anti-arrhythmics and the impact on outcome
The range of anti-arrhythmic agents prescribed to patients at the time of repeat ablation is displayed in Table 1. In the AI group, there were 11 patients (65%) that underwent medical de-escalation of AADs post redo ablation, while in the CF group, there were six patients (27%) who had medical de-escalation of AADs to maintain SR. Patients who underwent AI intervention had a statistically significant incidence of de-escalation in medical therapy post redo ablation procedure at 6 months follow-up (P = 0.02).
| Discussion | ▴Top |
Main findings
This is the first study to evaluate the impact of AI-guided intervention on redo PVI procedures in peAF. We have found that redo PVI, using either method, has been beneficial in maintaining SR in a subset of the study cohorts. Medical management was significantly de-escalated in the AI interventional group post-procedure. No intraprocedural or post-procedure complications occurred in either group. Although not reaching significance, there was a trend towards shorter procedure time in the AI group.
AI vs. CF outcomes
The PRAISE study has shown AI intervention to be effective in the treatment of peAF, with high rates of durable lesion formation and sustained SR at 1 year (93%) in their study [2]. Although AI had not demonstrated superiority in this treatment group, the study does highlight that a portion of these patients have benefited from a redo procedure with a significant percentage maintaining SR at 24 months in both groups.
Verma et al discussed the outcomes of PVI ablation alone vs. PVI plus additional ablation lines, specifically atrial roof and mitral isthmus. They found no difference in outcome at 24 months [14]. Szegedi et al reported that the impact of substrate modification with additional ablation lines was beneficial if performed by an experienced operator for the treatment of peAF [3]. In our study, the AI cohort had an increased incidence of additional ablation line creation during their redo PVI procedure. However, on examining a direct comparison of this subgroup, there was no significant difference between the maintenance of SR at 1 or 2 years.
Procedure details
The procedure details between the AI and CF groups were comparable. Pranata et al found in their systematic review that the ablation time was reduced with AI [12]. This was a trend in our cohort, despite the fact the electrophysiologists performed significantly more ablation lines in the AI group when compared to the CF group. Prior studies have reported shorter ablation times using AI, with comparable procedure time to CF [6, 15, 16]. A greater success rate in first-past PVI is also thought to contribute to shorter procedure time [17]. The comparable ablation and procedure times in this study could be attributed to the additional ablation lines created in the AI group.
Medical de-escalation
Casella et al recently published in a 24-month follow-up of primary PVI for PAF and peAF patients, that AI intervention was superior to CF regardless of anti-arrhythmic post-procedure [18]. This was in line with our study, where changes in anti-arrhythmic medication did not impact SR maintenance in either group. However, in our study, the AI group had significantly more patients undergoing medical de-escalation post redo ablation. This could indicate that the efficacy of using AI required less AADs to maintain SR; however, this is not conclusive.
Procedures details of complications
There were no complications reported in either group. This is in keeping with prior studies that have been carried out on AI intervention [15, 19, 20]. A systemic review carried out by Paranta et al comparing AI and CF head-to-head, found the complication rate among both procedures to be low [12]. There was no significant difference in the frequency of complication between either group, and this is reflected in our results and the current literature for both AI and CF [21].
Limitations
Our retrospective cohort has a limited number of patients due to a strict inclusion criterion to highlight the AI in redo ablations for peAF patients only. The study data were collected over 2 years and represents a heterogeneous time scale as the CF data were collected from procedures carried out from January 2016 to March 2017 and the AI procedure data were collected from June 2017 until August 2018. The heterogeneity in the study time is secondary to the uniform use of AI technology from June 2017 onwards based on the recommendations of the literatures and center policy to follow the new recommendations. Hence, AI was a replacement to FTI procedures.
The procedures were carried out by four different consultants and each patient was followed up by the consultant who carried out their procedure. The same consultants carried out the procedures in both the CF group and the AI group across both time periods to ensure consistent approach to each patient. The difference in consultant follow-up may have contributed to a confounding effect on medical de-escalation. However it is standard practice to de-escalate AADs if SR is maintained post procedure during follow-up. A prospective study would clarify this further. In addition the same consultants were involved in both the CF and AI procedures increasing consistency across both timelines.
Conclusion
This study demonstrated that the AI group had significant de-escalation of medical therapy in comparison to the FTI group. Despite the AI group trending towards improved procedures time, reduced radiation dose yet were not significant between both groups. Both technologies have a similar high safety profile and efficacy.
| Supplementary Material | ▴Top |
Suppl 1. Patient selection.
Acknowledgments
None to declare.
Financial Disclosure
Limited grant from J&J towards preparing and publishing the manuscript.
Conflict of Interest
Limited financial support from J&J to cover the publication fee of the manuscript.
Informed Consent
Written informed consent was obtained from all patients for their redo PVI.
Author Contributions
Sarah Jane Lennon and James Mannion: data collection, writing, data analysis; Edward Keelan, Jim O’Brien, and Gael Jauvert: important intellectual content and revisions; Usama Boles: Important intellectual content and revisions, supervisor, and final draft revisions.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, Boriani G, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373-498.
doi pubmed - Hussein A, Das M, Riva S, Morgan M, Ronayne C, Sahni A, Shaw M, et al. Use of ablation index-guided ablation results in high rates of durable pulmonary vein isolation and freedom from arrhythmia in persistent atrial fibrillation patients: the PRAISE study results. Circ Arrhythm Electrophysiol. 2018;11(9):e006576.
doi - Szegedi N, Geller L. New Results in Catheter Ablation for Atrial Fibrillation. In: Cismaru G, Chan KA (editor). Epidemiology and Treatment of Atrial Fibrillation. IntechOpen, Rijeka. 2019. Available from: https://www.intechopen.com/books/epidemiology-and-treatment-of-atrial-fibrillation/new-results-in-catheter-ablation-for-atrial-fibrillation.
- Hussein A, Das M, Chaturvedi V, Asfour IK, Daryanani N, Morgan M, Ronayne C, et al. Prospective use of Ablation Index targets improves clinical outcomes following ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2017;28(9):1037-1047.
doi pubmed - McLellan AJ, Ling LH, Azzopardi S, Lee GA, Lee G, Kumar S, Wong MC, et al. A minimal or maximal ablation strategy to achieve pulmonary vein isolation for paroxysmal atrial fibrillation: a prospective multi-centre randomized controlled trial (the Minimax study). Eur Heart J. 2015;36(28):1812-1821.
doi pubmed - Das M, Loveday JJ, Wynn GJ, Gomes S, Saeed Y, Bonnett LJ, Waktare JEP, et al. Ablation index, a novel marker of ablation lesion quality: prediction of pulmonary vein reconnection at repeat electrophysiology study and regional differences in target values. Europace. 2017;19(5):775-783.
doi pubmed - Neuzil P, Reddy VY, Kautzner J, Petru J, Wichterle D, Shah D, Lambert H, et al. Electrical reconnection after pulmonary vein isolation is contingent on contact force during initial treatment: results from the EFFICAS I study. Circ Arrhythm Electrophysiol. 2013;6(2):327-333.
doi pubmed - Kautzner J, Neuzil P, Lambert H, Peichl P, Petru J, Cihak R, Skoda J, et al. EFFICAS II: optimization of catheter contact force improves outcome of pulmonary vein isolation for paroxysmal atrial fibrillation. Europace. 2015;17(8):1229-1235.
doi pubmed - Phlips T, Taghji P, El Haddad M, Wolf M, Knecht S, Vandekerckhove Y, Tavernier R, et al. Improving procedural and one-year outcome after contact force-guided pulmonary vein isolation: the role of interlesion distance, ablation index, and contact force variability in the 'CLOSE'-protocol. Europace. 2018;20(FI_3):f419-f427.
doi pubmed - Koruth JS, Iwasawa J, Enomoto Y, Bar-Tal M, Ultchin Y, Sigal A, Mizrahi L, et al. Chamber-specific radiofrequency lesion dimension estimation using novel catheter-based tissue interface temperature sensing: a preclinical assessment. JACC Clin Electrophysiol. 2017;3(10):1092-1102.
doi pubmed - Nakagawa H, Ikeada A, Govari A, Papioannou T, Constantine G, Bar-Tal M, Silberschein E, et al. Prospective study using a new formula incorporating contact force, radiofrequency power and application time (Force-Power-Time Index) for quantifying lesion formation to guide long continuous atrial lesions in the beating canine heart. Circulation. 2013;128(22):Abstract 12104.
- Pranata R, Vania R, Huang I. Ablation-index guided versus conventional contact-force guided ablation in pulmonary vein isolation - Systematic review and meta-analysis. Indian Pacing Electrophysiol J. 2019;19(4):155-160.
doi pubmed - January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC, Jr., Ellinor PT, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS Guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the heart rhythm society. J Am Coll Cardiol. 2019;74(1):104-132.
doi pubmed - Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, Macle L, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812-1822.
doi pubmed - Solimene F, Schillaci V, Shopova G, Urraro F, Arestia A, Iuliano A, Maresca F, et al. Safety and efficacy of atrial fibrillation ablation guided by Ablation Index module. J Interv Card Electrophysiol. 2019;54(1):9-15.
doi pubmed - Munkler P, Kroger S, Liosis S, Abdin A, Lyan E, Eitel C, Eitel I, et al. Ablation index for catheter ablation of atrial fibrillation- clinical applicability and comparison with force-time integral. Circ J. 2018;82(11):2722-2727.
doi pubmed - Dhillon G, Ahsan S, Honarbakhsh S, Lim W, Baca M, Graham A, Srinivasan N, et al. A multicentered evaluation of ablation at higher power guided by ablation index: Establishing ablation targets for pulmonary vein isolation. J Cardiovasc Electrophysiol. 2019;30(3):357-365.
doi pubmed - Casella M, Dello Russo A, Riva S, Catto V, Negro G, Sicuso R, Cellucci S, et al. An ablation index operator-independent approach to improve efficacy in atrial fibrillation ablation at 24-month follow-up: a single center experience. J Interv Card Electrophysiol. 2020;57(2):241-249.
doi pubmed - Chelu MG, Morris AK, Kholmovski EG, King JB, Kaur G, Silver MA, Cates JE, et al. Durable lesion formation while avoiding esophageal injury during ablation of atrial fibrillation: Lessons learned from late gadolinium MR imaging. J Cardiovasc Electrophysiol. 2018;29(3):385-392.
doi pubmed - Futing A, Ruprecht U, Buchholz J, Bushmeier F, Reinsch N, Neven K. Use of Ablation Index significantly reduces the incidence of cardiac tamponade complicating pulmonary vein isolation for atrial fibrillation. Clin Res Cardiol. 2018;107(Suppl 3).
- Dagres N, Hindricks G, Kottkamp H, Sommer P, Gaspar T, Bode K, Arya A, et al. Complications of atrial fibrillation ablation in a high-volume center in 1,000 procedures: still cause for concern? J Cardiovasc Electrophysiol. 2009;20(9):1014-1019.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.