

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 15, Number 4, August 2024, pages 298-308

Does Sinus Rhythm Restoration in Patients With Atrial Fibrillation Undergoing Pulmonary Vein Isolation Have Acute Hemodynamic Benefits?
Tomo Komakia, c, Noriyuki Mohria, Akihito Ideishia, Kohei Tashiroa, Naoko Koyanagib, Shin-ichiro Miuraa, Masahiro Ogawaa, b
aDepartment of Cardiology, Fukuoka University Hospital, Fukuoka, Japan
bDepartment of Clinical Laboratory Medicine, Fukuoka University Faculty of Medicine, Fukuoka, Japan
cCorresponding Author: Tomo Komaki, Department of Cardiology, Fukuoka University Hospital, Fukuoka 814-0180, Japan
Manuscript submitted June 27, 2024, accepted August 12, 2024, published online August 20, 2024
Short title: SR Restoration in AF: Acute Hemodynamics
doi: https://doi.org/10.14740/cr1692
| Abstract | ▴Top |
Background: Although the restoration and maintenance of sinus rhythm (SR) in patients with atrial fibrillation (AF) have long-term benefits, few studies have investigated the acute hemodynamic benefits immediately after SR restoration. Therefore, we investigated whether hemodynamic changes occurred in the first few minutes after cardioversion from AF to SR.
Methods: We retrospectively enrolled 145 patients with AF and divided them into a pre-AF group comprising patients in whom SR was restored by electrical cardioversion during pulmonary vein isolation (PVI; n = 74) and a control group comprising patients who were in SR throughout the procedure (n = 71). The pre-AF group was subdivided into subgroups according to AF classification (paroxysmal AF (PAF), persistent AF (PerAF), and long-standing persistent AF (LSPAF)) and into quartiles based on the AF-heart rate (HR). The mean arterial pressure (MAP) and left atrial pressure (LAP) were measured immediately after transseptal puncture (pre-measurement) and before withdrawal from the left atrium after PVI (post-measurement). The changes in MAP and LAP between the pre- and post-measurement (ΔMAP and ΔLAP) were calculated by subtracting the pre-measurements (MAPpre and LAPpre) from the post-measurements (MAPpost and LAPpost).
Results: In the pre-AF group, the time from cardioversion to post-measurement was 19 ± 16 min. When ΔMAP and ΔLAP were compared with the control group, ΔMAP was significantly smaller (4.9 ± 17.8 vs. 11.0 ± 14.2 mm Hg, respectively; P = 0.025), and ΔLAP was not significantly different between the groups. In the subgroup analyses, although ΔLAP was not significantly different among AF types, ΔMAP was significantly increased in the PAF group compared to the PerAF and LSPAF groups (24.0 ± 18.5 vs. 3.1 ± 16.8 and 4.5 ± 18.1 mm Hg, respectively; P = 0.042). The HRpre in the quartiles with the lowest, second, third, and highest AF-HR were approximately 58, 74, 86, and 109 beats per minute (bpm), respectively. The ΔLAP and ΔMAP were not significantly different among the AF-HR quartile groups.
Conclusions: In patients with PAF, atrial contractions may resume quickly, which leads to hemodynamic improvement immediately after SR restoration. As for AF-HR, there was no significant impairment of ventricular diastolic filling at approximately < 109 bpm.
Keywords: Atrial fibrillation; Cardioversion; Mean arterial pressure; Left atrial pressure; Sinus rhythm
| Introduction | ▴Top |
Atrial contraction pumps blood into the ventricles, leading to increments in ventricular diastolic and stroke volumes [1, 2]. Atrial fibrillation (AF) decreases atrial contraction and can therefore reduce the stroke volume. Most researchers agree that loss of atrial contraction reduces cardiac output by 20% [3]. This effect may be particularly important in patients with reduced left ventricular compliance such as those with hypertrophic cardiomyopathy [4]. AF also causes an irregular rhythm and decreases the cycle length in a rapid ventricular response, which impairs optimal ventricular diastolic filling and reduces the stroke volume [5]. Uncontrolled persistent tachycardia can lead to a decrease in cardiac output and rate-related atrial and/or ventricular cardiomyopathy [6, 7]. These factors may contribute to adverse hemodynamic changes in patients with AF.
Cardioversion from AF to sinus rhythm (SR) optimizes ventricular diastolic filling because atrial contraction resumes and the cycle length increases, resulting in improved cardiac output [8, 9]. If SR can be maintained for a long period in patients with AF, it can stabilize neurohumoral activation and improve mitral regurgitation by decreasing the left atrial diameter and ventricular function, especially in patients with tachycardia-induced cardiomyopathy [10-12]. Rhythm control is very effective in improving symptoms and cardiac function in AF; therefore, the Japanese Circulation Society/Japanese Heart Rhythm Society 2021 guideline recommends catheter ablation for patients with AF and heart failure (recommendation class II a) [13-15].
To date, few studies have investigated the acute effects of cardioversion from AF to SR. We were interested in evaluating the changes in mean arterial pressure (MAP), as a surrogate marker for cardiac output, and left atrial pressure (LAP) immediately after restoration of SR. Therefore, we studied patients with AF who underwent pulmonary vein isolation (PVI) by radiofrequency catheter ablation (RFCA) in our hospital and investigated the acute hemodynamic effects by measuring the blood pressure, including the MAP and LAP, before and after cardioversion.
| Materials and Methods | ▴Top |
Study population
This retrospective, observational study included 145 consecutive patients with AF who underwent PVI by RFCA. The patients were enrolled at Fukuoka University Hospital, Fukuoka, Japan, between August 2019 and April 2023. Patients with drug-refractory AF, aged ≥ 18 years were included. Exclusion criteria were as follows: 1) additional intra-left atrial linear ablation and/or ablation of non-pulmonary vein triggers beyond PVI; 2) inadequate LAP measurements because of inadequate breath-holding; 3) insufficient perioperative data; 4) severe valvular disease; 5) maintenance hemodialysis for end-stage renal disease; 6) use of beta-agonists and/or adenosine triphosphate as provocative agents after PVI; 7) spontaneous change in heart rhythm from AF to SR or from SR to AF during the procedure; and 8) dependency on cardiac pacing with an implanted pacemaker.
The patients were divided into a pre-AF group, comprising those who had AF at the time they entered the cardiac catheterization laboratory that was reversed to SR by electrical cardioversion during PVI (n = 74), and a control group, comprising those who were in SR throughout the PVI procedure (n = 71). For subgroup analyses, we subdivided the pre-AF group into subgroups according to AF classification, that is, paroxysmal AF (PAF), persistent AF (PerAF), and long-standing persistent AF (LSPAF) and into quartiles according to the AF-heart rate (HR) and left atrial dimension (LAD). The AF type was determined according to the 2016 European Society of Cardiology guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardiothoracic Surgery [16]. PAF was defined as AF that reversed to SR within 7 days of occurrence, PerAF as AF that persisted for > 7 days after occurrence, and LSPAF as AF that persisted for longer than a year.
Ethical issues
This study was approved by the Institutional Review Board (U22-08-016) of Fukuoka University Hospital. All procedures of the present study were conducted in compliance with the Helsinki Declaration for research on human beings.
Clinical parameters
We collected admission data on age; sex; body mass index (BMI); comorbidities, including hypertension and diabetes mellitus; New York Heart Association (NYHA) functional class; laboratory tests, including hemoglobin, creatinine clearance, and B-type natriuretic peptide; and echocardiographic parameters, including LAD, left ventricular ejection fraction (LVEF); and heart failure and antiarrhythmic drugs taken before RFCA. HR and blood pressure, including systolic blood pressure (SBP), diastolic blood pressure (DBP), MAP, and LAP, were recorded twice during PVI; a pre-measurement was made immediately after entering the left atrium (LA) by transseptal puncture, and a post-measurement was made after completion of PVI, immediately before withdrawal from the LA. Data were also collected on the intraoperative amounts of intraprocedural fluid, sedatives (dexmedetomidine, fentanyl, diazepam, and thiopental), and contrast agents (in patients who underwent pulmonary vein angiography). The timing of electrical cardioversion during PVI was at the surgeon’s discretion and the time from cardioversion to post-measurement was recorded in the pre-AF group. The changes in HR and blood pressure between the pre- and post-measurements (ΔHR, ΔSBP, ΔDBP, ΔMAP, and ΔLAP) were calculated by subtracting the pre-measurements from the post-measurements.
Anesthesia management
All patients were sedated without intubation and administered oxygen at 2 L/min throughout the procedure under oxygen saturation and invasive blood pressure monitoring. Both diazepam 2.5 - 5 mg and fentanyl 0.05 mg were administered intravenously at the beginning of ablation. Dexmedetomidine was simultaneously administered by continuous infusion at an initial loading dose of 4 µg/kg/h over 10 min, followed by a maintenance dose at a rate of 0.4 µg/kg/h. The depth of sedation was assessed by the Bispectral Index® monitor (Aspect Medical Systems Inc, Natick, MA, USA), with a target value of 60 - 80. Depending on the patient’s pain and alertness during the procedure, diazepam and fentanyl were added, and the maintenance dose of dexmedetomidine was adjusted. In the pre-AF group, thiopental was additionally administered at a dose of 1 mg/kg for transient deep sedation immediately before electrical cardioversion.
RFCA
Antiarrhythmic drugs were discontinued in all patients for at least five half-lives before PVI. All patients underwent circumferential PVI with a ThermoCool® Surround Flow catheter (Biosense Webster, Diamond Bar, CA, USA) and the CARTO-3 mapping system (Biosense Webster, Diamond Bar, CA, USA). In this cohort, no additional substrate modifications beyond PVI were performed. In patients with redo AF, only the recurrent pulmonary vein potentials were isolated. After double transseptal puncture was performed by a radiofrequency needle, an SL-0 sheath (St. Jude Medical, St. Paul, MN, USA) and Agilis™ sheath (St. Jude Medical, St. Paul, MN, USA) were inserted into the LA. Pulmonary vein angiography was performed in most patients. Internal cardioversion was performed using a BeeAT catheter (Japan Lifeline, Tokyo, Japan) connected to a dedicated defibrillator (Shock AT; Japan Lifeline, Tokyo, Japan) to restore the SR. External cardioversion was performed in patients in whom the BeeAT catheter could not be placed in the coronary sinus. The timing of electrical cardioversion during PVI was at the surgeon’s discretion. During PVI, the pulmonary vein potentials were monitored using a ring catheter and the electrophysiological endpoint was a bidirectional conduction block between the LA and each PV. In patients with common atrial flutter, cavotricuspid isthmus isolation was performed after LA withdrawal during PVI.
Statistical analysis
Data were analyzed using the Stat Flex software (version 7.0; Artech Co., Ltd., Osaka, Japan). Continuous variables were expressed as mean ± standard deviation (SD) or median ± quartile deviation, and categorical variables were expressed as percentage (%). Continuous and categorical variables were compared between the two groups using Student’s t-test and Chi-square tests, respectively. When continuous variables did not show a normal distribution, we performed the Mann-Whitney U test. Continuous and categorical variables were compared among more than three groups by one-way analysis of variance and Chi-square analysis, respectively. When continuous variables did not show a normal distribution, we performed the Kruskal-Wallis test. Statistical significance was set at P < 0.05.
| Results | ▴Top |
Clinical characteristics in the pre-AF and control groups
In the entire group (N = 145), the mean age was 67 ± 9 years, and 102 of the patients (70%) were males. Table 1 shows the clinical characteristics of the pre-AF (n = 74) and control (n = 71) groups. The BMI was significantly higher in the pre-AF group than in the control group. Comorbidities including hypertension, diabetes mellitus, vascular disease, and stroke were not significantly different between the groups. Heart failure symptoms with NYHA functional class II were significantly more prevalent in the pre-AF group than in the control group. Patients in the pre-AF group had significantly higher hemoglobin and B-type natriuretic peptide levels, greater LAD, and lower LVEF than those in the control group. The uses of heart failure drugs including angiotensin-converting enzyme inhibitors, angiotensin receptor blocker, or angiotensin receptor neprilysin inhibitor, mineralocorticoid receptor antagonist, sodium-glucose cotransporter-2 inhibitor, and loop diuretics were not significantly different between the groups. Bepridil was used significantly less frequently in the pre-AF group than in the control group. In the entire group, 18% of patients (n = 26) were undergoing redo AF ablation; the frequency of redo AF was not significantly different between the groups. Cavotricuspid isthmus ablation for common atrial flutter was performed more frequently in the control group than in the pre-AF group.
 Click to view | Table 1. Clinical Characteristics in the Pre-AF and Control Groups |
Comparison of intraprocedural parameters between the pre-AF and control groups
Table 2 shows the intra-procedural parameters of both groups. HRpre was significantly higher in the pre-AF group than in the control group. Compared with the control group, the pre-AF group had significantly lower SBPpre and higher DBPpre and LAPpre. The amounts of intraprocedural fluid and sedatives other than thiopental (dexmedetomidine, fentanyl, and diazepam) administered during PVI were not significantly different between the two groups. Pulmonary vein angiography was performed in 135 patients (pre-AF group, n = 67 (91%); control group, n = 67 (94%)) and the amount of contrast agent used was not significantly different between the two groups. The time from cardioversion to post-measurement was 19 ± 16 min in the pre-AF group. The pre-AF group had significantly lower SBPpost and higher LAPpost than the control group.
Click to view | Table 2. Comparison of Intraprocedural Parameters Between the Pre-AF and Control Groups |
Hemodynamic changes immediately after SR restoration in the pre-AF group
Figure 1a shows the changes in the HR and blood pressure, including SBP, DBP, MAP, and LAP, 19 ± 16 min after cardioversion in the pre-AF group. Immediately after cardioversion, the HR was significantly lower and all blood pressure measurements other than DBP (SBP, MAP, and LAP) were significantly higher.
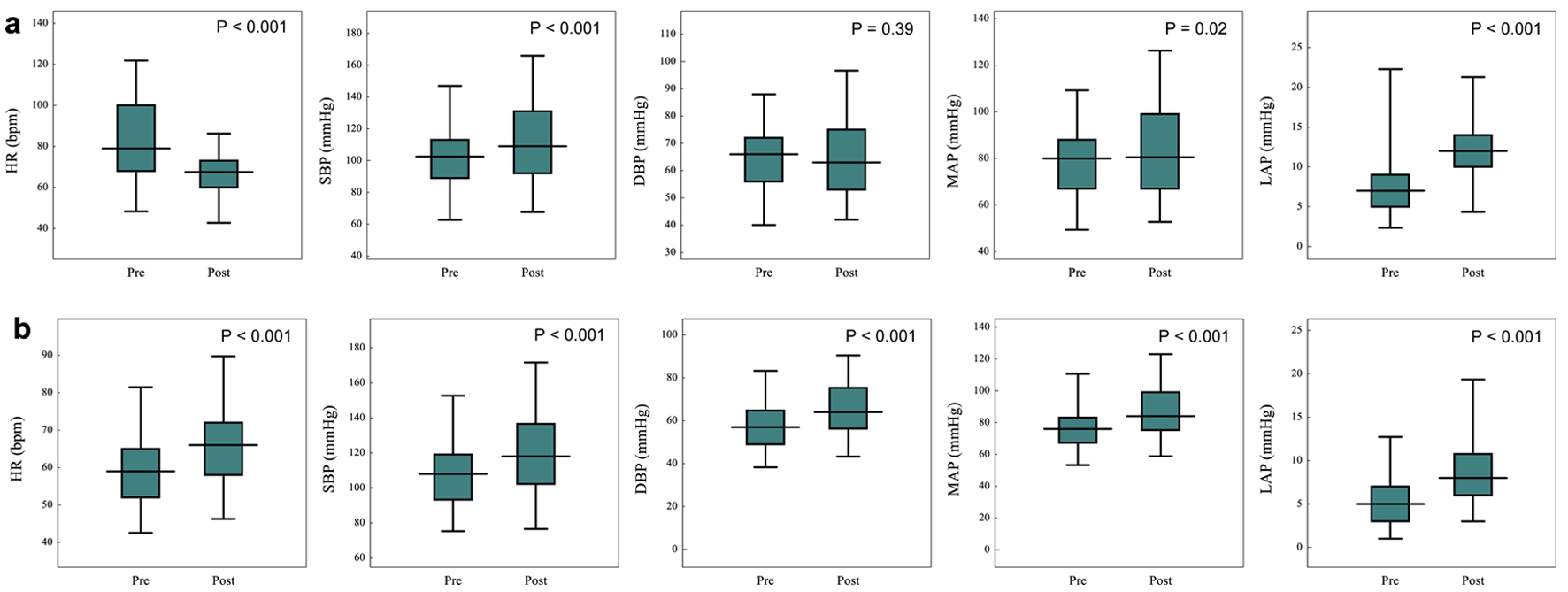 Click for large image | Figure 1. Changes in heart rate and blood pressure from before to 19 ± 16 min after sinus rhythm restoration in the pre-atrial fibrillation group (a) and from before to after pulmonary vein isolation in the control group (b). AF: atrial fibrillation; bpm: beats per minute; DBP: diastolic blood pressure; HR: heart rate; LAP: left atrial pressure; MAP: mean arterial pressure; SBP: systolic blood pressure. |
Hemodynamic changes after PVI in the control group
Figure 1b shows the changes in HR and blood pressure after PVI in the control group. The HR and all blood pressure measurements (SBP, DBP, MAP, and LAP) were significantly higher after PVI.
Comparison of the changes in HR (ΔHR) and blood pressure (ΔSBP, ΔDBP, ΔMAP, and ΔLAP) from before to after PVI between the pre-AF and control groups
Figure 2 compares the changes in HR and blood pressure from before to after PVI between the pre-AF and control groups. The pre-AF group showed a significantly greater decrease in HR than the control group (ΔHR, -16.3 ± 18.5 vs. 5.9 ± 9.1 beats per minute (bpm)), but the changes in SBP and LAP were not significantly different between the two groups. The pre-AF group showed a significantly lower increase in DBP and MAP than the control group (ΔDBP, 1.3 ± 13.4 vs. 8.8 ± 9.6 mm Hg; ΔMAP, 4.9 ± 17.8 vs. 11.0 ± 14.2 mm Hg).
 Click for large image | Figure 2. Comparison of the changes in heart rate and blood pressure from before to after pulmonary vein isolation in the pre-atrial fibrillation and control groups. AF: atrial fibrillation; bpm: beats per minute; ΔDBP: change in diastolic blood pressure; ΔHR: change in heart rate; ΔLAP: change in left atrial pressure; ΔMAP: change in mean arterial pressure; ΔSBP: change in systolic blood pressure. |
Comparison between the PAF, PerAF, and LSPAF groups
Table 3 shows the intraoperative parameters in the PAF (n = 5), PerAF (n = 48), and LSPAF (n = 21) groups. The mean duration of AF in the PAF group was 49.4 ± 34.7 h. The PAF group had a significantly higher HRpre and lower SBPpre, DBPpre, and MAPpre than the PerAF and LSPAF groups. The amounts of intraprocedural fluid, sedatives, and contrast agents administered during PVI were not significantly different between the three groups. The HRpost, SBPpost, DBPpost, MAPpost, and LAPpost were not significantly different between the three groups.
Click to view | Table 3. Comparison of Intraprocedural Parameters Among the AF Classification Groups |
Figure 3 shows a comparison of the changes in HR and blood pressure before and after PVI in the three groups. The PAF group showed a significantly greater decrease in HR (ΔHR, -26.6 ± 17.7 bpm) and increases in SBP (ΔSBP, 39.8 ± 26.9 mm Hg) and MAP (ΔMAP, 24.0 ± 18.5 mm Hg) than the PerAF and LSPAF groups.
 Click for large image | Figure 3. Comparison of changes in heart rate and blood pressure from before to after pulmonary vein isolation in patients with paroxysmal, persistent, and long-standing persistent atrial fibrillation. bpm: beats per minute; ΔDBP: change in diastolic blood pressure; ΔHR: change in heart rate; ΔLAP: change in left atrial pressure; LSPAF: long-standing persistent atrial fibrillation; ΔMAP: change in mean arterial pressure; PAF: paroxysmal atrial fibrillation; PerAF: persistent atrial fibrillation; ΔSBP: change in systolic blood pressure. |
Comparison among the AF-HR quartiles in the pre-AF group
Table 4 shows the intraprocedural parameters among the AF-HR quartile groups. The HRpre in the quartile with the lowest, second, third, and highest AF-HR were 57.7 ± 7.4, 74.0 ± 2.9, 86.1 ± 6.0, and 109.3 ± 8.1 bpm, respectively. None of the blood pressure parameters, including the SBPpre, DBPpre, MAPpre, or LAPpre were significantly different among the AF-HR quartiles. The amount of fentanyl used during the procedure differed significantly, but there were no significant differences in the amounts of other sedatives, contrast agents, or intraprocedural fluids among the AF-HR quartiles. The HRpost differed significantly, but all blood pressures, including the SBPpost, DBPpost, MAPpost, and LAPpost were not significantly different among the AF-HR quartiles.
Click to view | Table 4. Comparison of Intraprocedural Parameters Among the Quartile AF-HR Groups |
Figure 4 compares the changes in HR and blood pressure before and after PVI among the AF-HR quartiles. Although the HR decreased significantly more in the quartile with the highest AF-HR than in the quartile with the lowest, second, and third AF-HR (ΔHR; -37.2 ± 9.4 vs. 3.8 ± 12.6, -9.6 ± 10.6, and -19.9 ± 10.2 bpm, respectively), the changes in ΔSBP, ΔDBP, ΔMAP, and ΔLAP were not significantly different among the AF-HR quartiles.
 Click for large image | Figure 4. Comparison of the changes in heart rate and blood pressure from before to after pulmonary vein isolation in patients with the quartiles of atrial fibrillation-heart rate. bpm: beats per minute; ΔDBP: change in diastolic blood pressure; ΔHR: change in heart rate; ΔLAP: change in left atrial pressure; ΔMAP: change in mean arterial pressure; Q: quartile; ΔSBP: change in systolic blood pressure. |
Comparison among the LAD quartiles in the pre-AF group
Table 5 shows the intraprocedural parameters among the LAD quartile groups. The LAD in quartile with the lowest, second, third, and highest LAD were 37.0 ± 2.9, 41.8 ± 0.8, 45.2 ± 1.3, and 51.3 ± 3.1 mm, respectively. The HRpre differed significantly, but there were no significant differences in the blood pressure parameters, including the SBPpre, DBPpre, MAPpre, and LAPpre among the LAD quartiles. There were no significant differences in the amounts of intraprocedural fluids, sedatives, or contrast agent among the LAD quartiles. The LAPpost differed significantly, but the HRpost and the other blood pressures, including the the SBPpost, DBPpost, and MAPpost were not significantly different among the LAD quartiles.
Click to view | Table 5. Comparison of Intraprocedural Parameters Among the Quartile LAD Groups |
Figure 5 compares the changes in HR and blood pressure before and after PVI among the LAD quartiles. The changes in ΔHR, ΔSBP, ΔDBP, ΔMAP, and ΔLAP were not significantly different among the LAD quartiles.
 Click for large image | Figure 5. Comparison of the changes in heart rate and blood pressure from before to after pulmonary vein isolation in patients with the quartiles of left atrial dimension. bpm: beats per minute; ΔDBP: change in diastolic blood pressure; ΔHR: change in heart rate; ΔLAP: change in left atrial pressure; ΔMAP: change in mean arterial pressure; Q: quartile; ΔSBP: change in systolic blood pressure. |
| Discussion | ▴Top |
We investigated the acute hemodynamic effects of SR restoration in patients with AF. As the MAP is determined by cardiac output and peripheral vascular resistance, we used it as a surrogate marker for cardiac output. We were also interested in the change of LAP immediately after cardioversion from AF to SR.
The main findings in this study were as follows. First, hemodynamics could improve immediately after SR restoration in patients with PAF. Compared the pre-AF group including all AF types with the control group, there were no significant differences in the changes of MAP and LAP just after SR restoration. We subdivided the pre-AF group according to AF classification and the mean duration of AF in the PAF group was 49.4 ± 34.7 h, which was relatively short duration. When compared among these groups, there was no significant difference in the change of LAP among the groups, but the PAF group showed a significant increase in MAP than the PerAF and LSPAF groups. As the recovery of atrial mechanical function depends on the duration of AF before cardioversion [17], atrial contractions may resume quickly in short duration of AF. As a result, the hemodynamics of the PAF patients improved immediately after SR restoration, whereas those of the PerAF and LSPAF patients did not improve because atrial contractions had not yet resumed. Second, there was no significant impairment of ventricular diastolic filling when AF-HR was at approximately < 109 bpm. To investigate the hemodynamic effects of AF-HR, we subdivided the pre-AF group into quartiles according to AF-HR. Compared among the AF-HR quartiles, there were no significant hemodynamic differences among these groups. Previously, in the RACE II (Rate control efficacy in permanent atrial fibrillation: a comparison between lenient versus strict rate control II) study, Van Gelder et al compared major cardiovascular events in patients with AF treated by a lenient (resting HR < 110 bpm) or strict rate-control strategy (resting HR < 80 bpm and HR during moderate exercise < 110 bpm) [18]. The group hypothesized that the lenient rate-control strategy might induce or worsen heart failure, but the results showed that the lenient strategy was not inferior to the strict strategy. Although the authors did not explain why the lenient rate-control strategy was non-inferior, our findings suggest that this was because neither rate-control strategy caused significant impairment of ventricular diastolic filling. Lastly, the LAD was also significantly different as well as the proportion of AF types and AF-HR (HRpre) in comparison of baseline characteristics between the pre-AF group and the control group. As these factors may become confounding factors in the result, we also subdivided the pre-AF group according to the LAD quartiles. But there were no significant hemodynamic differences among the quartile LAD groups, which did not seem to be a confounding factor in the result.
This study had several limitations. First, this study was limited by its retrospective design. Although the patients who met the inclusion criteria of this study were consecutively enrolled between August 2019 and April 2023 in our hospital, there was a selection bias by retrospective design. Second, the subgroups of patients according to AF types, AF-HR quartiles, and LAD quartiles were small; therefore, the statistical power was low, and additional investigations with larger sample sizes are necessary to confirm the results of subgroup analyses. Third, most patients enrolled in the pre-AF group had preserved LVEF (mean ± SD, 59.3 ± 9.6%) and stable heart failure symptoms (NYHA functional class I, 50%; class II, 50%). Therefore, this study does not provide information on the acute hemodynamic benefits of SR restoration in patients with AF with significantly different characteristics from those enrolled in this study, such as those with depressed LVEF, more severe symptoms (NYHA functional class III/IV), and/or a more rapid ventricular response, and additional investigations are warranted. Forth, thiopental was administered intravenously before electrical cardioversion in the pre-AF group but not throughout the procedure in the control group. Although the dose of thiopental used in the pre-AF group was 1.3 ± 0.6 mg/kg, which was considerably less than the usual dose (3 - 4 mg/kg), it could potentially influence the MAPpost and LAPpost in the pre-AF group and become a confounding factor in the results. However, because electrical cardioversion is extremely painful for patients, the use of an additional intravenous anesthetic is unavoidable. In clinical practice, electrical cardioversion is often performed using the same protocol as that used in this study; therefore, we believe that these data can also be applied in clinical settings. Finally, in the pre-AF group, SR restoration was established by internal cardioversion in all patients except for one in whom external cardioversion was performed because of difficulties in placing a 7-Fr electrode catheter in the coronary sinus. In contrast, the control group did not undergo electrical cardioversion because their heart rhythms were SR throughout the procedure. Internal and external cardioversions decrease the left atrial chamber and appendage function [19], which may explain why the LAP was unchanged in the pre-AF group. This problem is difficult to resolve because it is difficult to record a large amount of data on patients with AF who spontaneously return to SR without cardioversion.
Conclusions
In patients with PAF, atrial contractions may resume quickly, which leads to hemodynamic improvement immediately after cardioversion. As for AF-HR, there was no significant impairment of ventricular diastolic filling at approximately < 109 bpm.
Acknowledgments
None to declare.
Financial Disclosure
There was no specific funding source to be mentioned.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
The requirement for informed consent was waived due to the retrospective nature of the study.
Author Contributions
TK was involved in the conceptualization, design, supervision, and analysis of the study and manuscript writing. SM and MO supervised and conducted the analyses, and approved the final manuscript. NM, AI, KT, and NK analyzed and approved the final manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Rahimtoola SH, Ehsani A, Sinno MZ, Loeb HS, Rosen KM, Gunnar RM. Left atrial transport function in myocardial infarction. Importance of its booster pump function. Am J Med. 1975;59(5):686-694.
doi pubmed - Linderer T, Chatterjee K, Parmley WW, Sievers RE, Glantz SA, Tyberg JV. Influence of atrial systole on the Frank-Starling relation and the end-diastolic pressure-diameter relation of the left ventricle. Circulation. 1983;67(5):1045-1053.
doi pubmed - Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA, Weyman AE. Atrial enlargement as a consequence of atrial fibrillation. A prospective echocardiographic study. Circulation. 1990;82(3):792-797.
doi pubmed - Bonow RO, Frederick TM, Bacharach SL, Green MV, Goose PW, Maron BJ, Rosing DR. Atrial systole and left ventricular filling in hypertrophic cardiomyopathy: effect of verapamil. Am J Cardiol. 1983;51(8):1386-1391.
doi pubmed - Daoud EG, Weiss R, Bahu M, Knight BP, Bogun F, Goyal R, Harvey M, et al. Effect of an irregular ventricular rhythm on cardiac output. Am J Cardiol. 1996;78(12):1433-1436.
doi pubmed - Zipes DP. Atrial fibrillation. A tachycardia-induced atrial cardiomyopathy. Circulation. 1997;95(3):562-564.
doi pubmed - Redfield MM, Kay GN, Jenkins LS, Mianulli M, Jensen DN, Ellenbogen KA. Tachycardia-related cardiomyopathy: a common cause of ventricular dysfunction in patients with atrial fibrillation referred for atrioventricular ablation. Mayo Clin Proc. 2000;75(8):790-795.
doi pubmed - Rodman T, Pastor BH, Figueroa W. Effect on cardiac output of conversion from atrial fibrillation to normal sinus mechanism. Am J Med. 1966;41(2):249-258.
doi pubmed - Raymond RJ, Lee AJ, Messineo FC, Manning WJ, Silverman DI. Cardiac performance early after cardioversion from atrial fibrillation. Am Heart J. 1998;136(3):435-442.
doi pubmed - Roy D, Paillard F, Cassidy D, Bourassa MG, Gutkowska J, Genest J, Cantin M. Atrial natriuretic factor during atrial fibrillation and supraventricular tachycardia. J Am Coll Cardiol. 1987;9(3):509-514.
doi pubmed - Gertz ZM, Raina A, Saghy L, Zado ES, Callans DJ, Marchlinski FE, Keane MG, et al. Evidence of atrial functional mitral regurgitation due to atrial fibrillation: reversal with arrhythmia control. J Am Coll Cardiol. 2011;58(14):1474-1481.
doi pubmed - Viswanathan K, Daniak SM, Salomone K, Kiely T, Patel U, Converso K, Manning WJ, et al. Effect of cardioversion of atrial fibrillation on improvement in left ventricular performance. Am J Cardiol. 2001;88(4):439-441.
doi pubmed - Alam M, Thorstrand C. Left ventricular function in patients with atrial fibrillation before and after cardioversion. Am J Cardiol. 1992;69(6):694-696.
doi pubmed - Hsu LF, Jais P, Sanders P, Garrigue S, Hocini M, Sacher F, Takahashi Y, et al. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004;351(23):2373-2383.
doi pubmed - Nogami A, Kurita T, Kusano K, Goya M, Shoda M, Tada H, Naito S, et al. JCS/JHRS 2021 guideline focused update on non-pharmacotherapy of cardiac arrhythmias. J Arrhythm. 2022;38(1):1-30.
doi pubmed pmc - Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893-2962.
doi pubmed - Manning WJ, Silverman DI, Katz SE, Riley MF, Come PC, Doherty RM, Munson JT, et al. Impaired left atrial mechanical function after cardioversion: relation to the duration of atrial fibrillation. J Am Coll Cardiol. 1994;23(7):1535-1540.
doi pubmed - Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, Hillege HL, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
doi pubmed - Omran H, Jung W, Rabahieh R, Schimpf R, Wolpert C, Hagendorff A, Fehske W, et al. Left atrial chamber and appendage function after internal atrial defibrillation: a prospective and serial transesophageal echocardiographic study. J Am Coll Cardiol. 1997;29(1):131-138.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.